Efficacy and Safety of Small Molecule Water in Patients with Asymptomatic Hyperuricemia: A Multicenter, Randomized, Double-blind, Placebo-controlled Trial
Abstract
Background: To date, there is no appropriate scheme to lower Serum Uric Acid (SUA) in patients with SUA between 7.0-9.0 mg/dL without symptoms and comorbidities. We wondered whether Small Molecule Water (SMW) lower SUA in these patients.
Methods: This multicenter, randomized, double-blind, placebo-controlled trial was conducted at six tertiary hospitals in China. Participants aged at least 18 years with asymptomatic hyperuricemia who had no comorbidities were screened. Patients were randomly assigned (1:1) to either SMW (1600 ml/day, intervention) or placebo (raw water, 1600ml/day, control), simultaneously recommending to follow a conventional low-purine (i.e., plant-dominant low-protein) diet. The primary outcome was the mean change of SUA from baseline to 12 weeks.
Results: 232 participants were enrolled from 6 tertiary hospitals. Mean SUA decreased by 0.71 mg/dL (95% CI 0.37-1.03 mg/dL) from baseline to 12 weeks in the intervention group and by 0.36 mg/dL (95% CI 0.26-0.45 mg/dL) in the control group, with a group difference of 0.35 mg/dL (95% CI 0.25-0.35 mg/dL; p<0∙0001). At 12 weeks, 44 (35.3%) of 116 patients in the intervention group and 24 (20.7%) of 116 patients in the control group had an SUA of less than 7.0 mg/dl, with a relative risk of 1.71 (95% CI 1.33-2.14). Also, body mass index, total cholesterol, and low-density lipoprotein cholesterol decreased, but high-density lipoprotein cholesterol increased in the intervention group.
Conclusion: SMW may short-termly lower SUA and improve body metabolism in adult patients with asymptomatic hyperuricemia on a conventional low-purine diet.
Serum uric acid; Asymptomatic hyperuricemia; Small molecule water
INTRODUCTION
Hyperuricemia refers to the fasting blood uric acid level exceeding 7.0 mg/dL in adults, regardless of gender, twice on different days on a normal purine diet [1]. Although clinically relevant manifestations may develop in a hyperuricemic individual at any point, about two-thirds or more of such individuals remain asymptomatic, never developing gout flares, tophaceous gout, acute or chronic hyperuricemic nephropathy, or uric acid nephrolithiasis [2,3]. Asymptomatic hyperuricemia is a term traditionally applied to settings where the serum urate concentration is elevated but in which neither symptoms nor signs of monosodium urate crystal deposition disease, such as gout or uric acid renal disease, have occurred. In addition to its relationship with urate or uric acid crystal deposition, asymptomatic hyperuricemia has also been associated with other disorders that appear to be largely unrelated to crystal deposition, including hypertension, chronic kidney disease, cardiovascular disease, and insulin resistance syndrome. Our previous studies reported that asymptomatic hyperuricemia was associated with adverse cardiovascular disease in elderly patients without comorbidities [4-6]. A five-year Japanese cohort study also found that asymptomatic hyperuricemia carried a significant risk of developing cardiometabolic conditions in Japanese individuals without comorbidities [7].
For patients with asymptomatic hyperuricemia and no comorbidities such as hypertension, chronic kidney disease, cardiovascular disease, or nephrolithiasis, Serum Uric Acid (SUA)>9.0 mg/dL should be intervened with urate-lowering drugs, with a target of 7.0 mg/dL.1 Thus, it is a challenge for clinical medical workers to long-termly keep SUA<7.0 mg/dL in patients without comorbidities with SUA between 7.0-9.0 mg/ dL without drug intervention.
Natural water is a flexible and dynamic water cluster, which usually contains 10-13 molecules, about 110-130 Hz. These water molecules are linked to each other by a hydrogen bond network [8,9]. More hydrogen-bonded network structure increases viscosity, reduces diffusivities, and lowers active participation of water molecules, which slows the biological and chemical reactions [8,9]. Any factors that reduce hydrogen bonding and hydrogen bond strength should encourage water activity. When the magnetic field is applied to normal water, the water molecules are restructured into tiny water molecule clusters called Small Molecules Water (SMW) that contain 5-7 water molecules and less than 100 Hz, which can rapidly penetrate human tissues and cells, to enhance nutrient replenishment and waste discharge, promote metabolism, thereby enhancing metabolic function.10 A recent study reported that SMW may retard crystal formation, reduce urinary calcium and phosphorus excretion and promote earlier OPN mRNA expression in the rat kidney [10]. Based on these findings, we wanted to know whether SMW may have a particular impact on the human body's uric acid metabolism. Thus, we hypothesized that SMW reduced SUA in patients with asymptomatic hyperuricemia (serum uric acid between 7.0-9.0 mg/dL).
MATERIALS AND METHODS
Study design and participants
The multicenter, randomized, double-blind, placebo-controlled trial in 6 tertiary hospitals in China was conducted from 2023-02-01 to 2023-04-30. The study was approved by the committee for medical and health research ethics of Shanghai Jiao Tong University affiliated sixth people's hospital, Zhejiang University Medical College affiliated Sir Run Run Shaw Hospital, the second affiliated hospital of Guangzhou Medical University, Zhujiang Hospital of Southern Medical University, the first affiliated hospital of Nanchang University, and General Hospital of Ningxia (ethics approval number: 2022-133). Medical University via. a centralized institutional review board review process. In this multicenter study, the Committee for Medical and Health Research Ethics of Shanghai Jiao Tong University Affiliated Sixth People's Hospital served as a central institutional review board. The trial was done in accordance with the declaration of helsinki guidelines on good clinical practice. Written informed consent was given by all participants at screening visits. An independent data and safety monitoring board monitored the progress of the trial and reviewed safety and effectiveness data during the trial. Written informed consents were obtained from all participants.
Critical inclusion criteria included adult participants (≥ 18 years) with asymptomatic hyperuricemia inadequately controlled with diet and exercise alone. Eligible participants had an SUA of 7.0-9.0 mg/dL at screening (recruiting time: from 2022-11 17 to 2023-01-31), with stable weight (no change outside of 5%) during the previous three months with an agreement to not initiate a diet or exercise program during the study with the intent of reducing body weight other than the lifestyle and dietary measures for hyperuricemia treatment. Additionally, per the protocol (supplemental materials), sites needed to educate participants on hyperuricemia management, including management of general counseling on diet and exercise. Critical exclusion criteria included history of gout, complications of hyperuricemia, hypertension, abnormal lipid metabolism, diabetes, stroke, coronary heart disease, cardiac insufficiency, uric acid nephrolithiasis, renal function damage (estimated glomerular filtration rate <60 mL/min/1.73m²), use of uric acid lowering drugs, thiazide diuretics or other drugs that affect uric acid within four weeks of entering this study, pregnancy status, patients with malignant tumors, life expectancy less than six months, refusal to sign the informed consent form.
Randomization and masking
Participants were randomly assigned (1:1) to receive four bottles of SMW (1600 ml/day, Shanghai Taihe Water Environment Technology Development Co., Ltd., the intervention group) or a placebo (raw water, 1600ml/day, Shanghai Taihe Water Environment Technology Development Co., Ltd., the control group). All bottles were similar in appearance. Assignment to the treatment group was determined by a computer-generated random sequence using the Eli Lilly and Company interactive web-response system. This system is externally validated and compliant with the Code of Federal Regulations 21, part 11. All participants, investigators, and the sponsor were masked to treatment assignment. The randomization data was only assessed by a minimal group of personnel (interactive web-response system support team, Data Movement Group associates, demand forecasters and clinical supply coordinators). Additionally, when they finish 1600 ml of experimental water, all participants can consume 400ml-800 ml of raw water again, depending on their willingness.
Procedures
Participants in both groups were instructed to a conventional low-purine diet (i.e., plant-dominant low-protein) at the start of the treatment, based on the advice of a clinical dietitian. Participants were seen every two weeks for water dispensing and every month for detailed assessments. Assessments included laboratory tests, periodic questionnaires, vital signs, and adverse events. Investigators were advised to promote a healthy lifestyle and to manage SUA concentrations according to guidelines. They were free to add any SUA-lowering drugs when levels of SUA were more than 9.0 mg/dl. Management of blood pressure, lipids, other cardiovascular risk factors, and medical conditions was at the discretion of the study investigator or the patient's usual physician(s) as informed by current guidelines. Unless consent was explicitly withdrawn, all randomly assigned participants were followed up until the end of the trial, irrespective of adherence to study medication. Those who stopped the study intervention were encouraged to restart it unless there was a clear contraindication. Study data were collected at baseline and every 2-week follow-up visit by trained, certified research staff. At a central clinical laboratory, an overnight fasting blood sample was collected at the baseline visit to measure laboratory measurements.
Participants’ baseline demographic and characteristics and laboratory variables were recorded: Age, sex, Body Mass Index (BMI), education (high school or lower/college or higher), cigarette smoking (never smoked, former smokers [quit], and current smokers [who smoke either everyday or some days]), alcohol drinking [who drink either everyday or some days], regular physical activity [who excise for at least 30 minutes either everyday or >=3 times/week], duration of hyperuricemia, and laboratory measurements (SUA, glomerular filtration rate [eGFR], total cholesterol, High Density Lipoprotein Cholesterol [HDL-C], and low density lipoprotein cholesterol [LDL-C]). eGFR was measured using the chronic kidney disease epidemiology collaboration creatinine equation.
Study participants’ identification information and other data were double entered at the study and data coordinating center at Shanghai Jiao Tong University Affiliated Sixth People's Hospital.
Raw water (placebo, daily drinking water) was transported to the multi-media filter tank through the pipeline and entered the 5-micrometer-specific precision filter. After the specific precision f ilter, water entered the 0.2-micrometer specific ultrafiltration membrane filter. Then, SMW was constructed with 5-7 water molecules and less than 90 Hz.
Outcomes and definitions
The primary outcome was the mean change of SUA from baseline to 12 weeks. The secondary outcome was the proportion of patients with an SUA of less than 7.0 mg/dl at 12 weeks, the mean change of total cholesterol, HDL-C, LDL-C, and body BMI. Complications of hyperuricemia such as gout and nephrolithiasis were recorded during follow-up.
The Chinese guidelines for the diagnosis and treatment of hyperuricemia and gout (2023) define the diagnostic criteria for hyperuricemia as follows: Regardless of sex, the fasting SUA level is measured twice on two different days, and hyperuricemia is when the SUA level is more than 7.0 mg/dL. Gout events were recorded, characterized by sudden, severe pain attacks, swelling, redness, and tenderness in one or more joints, most often in the big toe. A conventional low-purine diet was defined as a plant dominant low-protein diet of 0.8 g/kg/day composed of >50% plant-based sources, which was promising and consistent with the precision nutrition [11].
Statistical analysis
To achieve 90% power for demonstrating the superiority of the intervention group to the controlled group in change from baseline for SUA at Week 12, a sample size of 208 participants was required, randomly assigned in a 1:1 ratio to the intervention group and the controlled group. This assumes an actual treatment difference of 0.3 mg/dL with a typical Standard Deviation (SD) of 0.65 mg/dL for the change in SUA from baseline based on our previous data analysis (pre-trial data). Additionally, we considered the 10% missing primary outcome data due to loss of contact and other factors. A total of 232 participants were included. The statistical power was calculated on the basis of a bilateral T-test with PASS software.
All efficacy and safety analyses were done according to an intention-to-treat approach that included all randomly assigned participants irrespective of adherence. Mean differences in mean SUA changes between the intervention and control groups were tested using a linear mixed-effects model. An autoregressive correlation structure was selected for these repeated measures. The model term included fixed effects of treatment, baseline value (continuous), visit, and the interaction of treatment-by visit., as well as participant as a random effect [12]. Fisher's exact test was used to examine the treatment difference in categorical outcomes. Relative risks with 95% CI were calculated using the log-binomial model for the categorical variables. A set of plausible ranges for laboratory tests was defined before unblinding, and tests with values outside these ranges were excluded from the analyses. In these analyses, pairwise deletion of missing data was used to preserve all information observed. Additionally, multiple imputations for missing data in the multivariable analyses were conducted using the Markov chain Monte Carlo method with an arbitrary missing pattern, assuming a normal multivariate distribution [13]. All statistical analyses were done by two biostatisticians in duplicate using Stata 16.0 statistical software (StataCorp, College Station, TX). The two biostatisticians were masked to each other’s SAS codes but not to randomization assignment.
RESULTS
Participant disposition
Two hundred thirty-two participants were randomized in a 1:1 ratio to the intervention or control groups (Figure 1). The last 12-week follow-up visit was conducted on April 20, 2023. During the 12 weeks, 3 participants discontinued to study treatment, one discontinued to study in the intervention group, one discontinued to study treatment, and one discontinued to study in the control group due to no SUA change. Additionally, 5 of the 116 participants in the intervention group and 3 of the 116 in the control group had missing data on lipids at the 12-week follow-up visit.
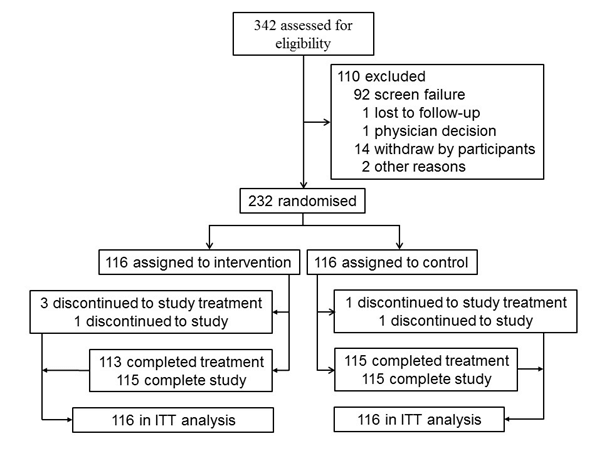
Figure 1:Trial profile.
Baseline demographic characteristics
On average, the study participants were 30.5 ± 8.4 years old, 199 (85.8%) were male, and the median duration of hyperuricemia was 5.6 years (IQR 4-11 years). The mean SUA level was 7.93 ± 0.68 mg/dL in the cohort study. The baseline and demographic characteristics were comparable across both groups (Table 1).
| Characteristics | Intervention | Control |
|---|---|---|
| Number of participants | 116 | 116 |
| Age, years | 30.5 ± 8.6 | 30.5 ± 8.4 |
| Sex | ||
| Male | 109 (94.0%) | 110 (94.8%) |
| Female | 7 (6.0%) | 6 (5.2%) |
| BMI, kg/m2 | 25.9 ± 3.9 | 26.3 ± 3.6 |
| Education | ||
| High school or lower | 71 (61.2%) | 69 (59.5%) |
| College or higher | 45 (38.8%) | 47 (40.5%) |
| Cigarette smoking | ||
| Never smoked | 79 (68.1%) | 80 (69.0%) |
| Former smokers | 4 (3.4%) | 5 (4.3%) |
| Current smokers | 33 (28.4%) | 31 (26.7%) |
| Weekly alcohol drinking | 39 (33.6%) | 37 (31.9%) |
| Physical activity ≥5 times per week | 29 (25.0%) | 28 (24.1) |
| Duration of hyperuricemia, years | 5.5 ± 1.1 | 5.7 ± 1.2 |
| Laboratory measurements | ||
| SUA, mg/dL | 7.93 ± 0.72 | 7.93 ± 0.66 |
| eGFR, mL/min per 1.73 m2 | 103.4 ± 25.0 | 100.3 ± 20.8 |
| Total cholesterol, mg/dL | 210.9 ± 33.8 | 205.2 ± 32.5 |
| LDL-c, mg/dL | 46.1 ± 11.9 | 47.0 ± 11.4 |
| HDL-c, mg/dL | 137.7 ± 27.8 | 133.8 ± 25.4 |
| Note: BMI: Body Mass Index; SUA: Serum Uric Acid; eGFR: estimated Glomerular Filtration Rate; LDL-C: Low Density Lipoprotein Cholesterol; HDL-C: High Density Lipoprotein Cholesterol. | ||
Table 1: Summary of selected baseline and demographic characteristics in the randomized population.
Efficacy
Primary endpoint: Table 2 showed the effectiveness of the SMW intervention versus the raw water on outcomes. Both groups showed a statistically significant (p< 0.001) reduction in SUA from baseline to week 12(the intervention group, 0.71 mg/dL [95% CI 0.37-1.03 mg/dL]; the control group, 0.36 mg/dL [0.26-0.45 mg/dL]). At week 12, participants showed a significantly higher mean reduction in SUA from baseline when treated with SMW versus raw water (mean difference, 0.35 mg/dL, 0.25-0.53 mg/dL, p < 0.001). The reduction was observed from week 4 through Week 12 (Figure 2).
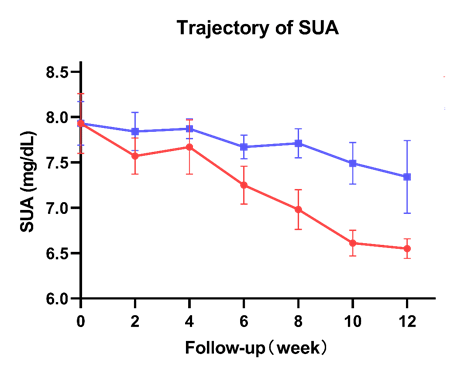
Figure 2: Mean change of SUA. Note: ( ): Small molecule water group; (
): Small molecule water group; ( ): Control group; SUA: Serum Uric Acid.
): Control group; SUA: Serum Uric Acid.
Secondary endpoints: At 12 weeks, 44 (35.3%) of 116 patients in the intervention group and 24 (20.7%) of 116 patients in the control group had an SUA of less than 7.0 mg/dL, with a risk difference of 1.71 (95% CI 1.33-2.14) (Table 2).
| Variables | Proportion or mean change (95% CI) | Net or risk difference (95% CI) | p-value | |
|---|---|---|---|---|
| Intervention | Control | |||
| Primary outcome | ||||
| Mean change in SUA from baseline to 12 weeks, mg/dL | 0.71 (0.37-1.03) | 0.36 (0.26-0.45) | 0.35 (0.25-0.53) | <0.001 |
| Secondary outcomes | ||||
| Proportion of participants with SUA < 7.0 mg/dL at 12 weeks | 35.3% (17.6-60.8) | 20.7% (13.2-28.4) | 1.71 (1.33-2.14)* | <0.001 |
| Change in total cholesterol from baseline to 12 weeks, mg/dL | 23.1 (12.4-36.2) | 7.6 (2.2-12.5) | 15.5 (6.8-24.8) | <0.001 |
| Change in LDL-c from baseline to 12 weeks, mg/dL | 7.9 (3.3-10.8) | 1.5 (0.7-4.3) | 6.4 (3.1-9.8) | <0.001 |
| Change in HDL-c from baseline to 12 weeks, mg/dL | 11.1 (7.3-15.6) | 5.3 (3.2-8.0) | 5.8 (2.8-8.9) | <0.001 |
| Change in BMI from baseline to 12 weeks, kg/m2 | 1.6 (1.0-2.4) | 0.6 (9 0.2-1.1) | 1.0 (0.4-1.8) | 0.016 |
| Note: (*): Adjusted for age, sex, Body Mass Index (BMI), lab variables, and centers; SMW: Small Molecule Water; SUA: Serum Uric Acid; LDL-C: Low-Density Lipoprotein-Cholesterol; HDL-C: High-Density Lipoprotein-Cholesterol. CI: Confidence Index. | ||||
Table 2: Effectiveness of the SMW intervention vs. raw water on outcomes among 232 participants.
Mean total cholesterol decreased by 23.1 mg/dL (95% CI 12.4 36.2 mg/dL) from baseline to 12 weeks in the intervention group and by 7.6 mg/dL (95% CI 2.2-12.5 mg/dL) in the control group, with a group difference of 15.5 mg/dL (95% CI 6.8- 24.8 mg/dL; p<0∙0001) (Figure 3). Mean HDL-C increased by 11.1 mg/ dl (95% CI 7.3-15.6 mg/dL) from baseline to 12 weeks in the intervention group and by 5.3 mg/dL (95% CI 3.2-8.0 mg/dL) in the control group, with a group difference of 5.8 mg/dL (95% CI 2.8-8.9 mg/dL; p<0∙0001) (Figure 4). Mean LDL-C decreased by 7.9 mg/dL (95% CI 3.3-10.8 mg/dL) from baseline to 12 weeks in the intervention group and by 1.5 mg/dL (95% CI 0.7 4.3 mg/dL) in the control group, with a group difference of 6.4 mg/dL (95% CI 3.1-9.8 mg/dL; p<0∙0001) (Figure 5).
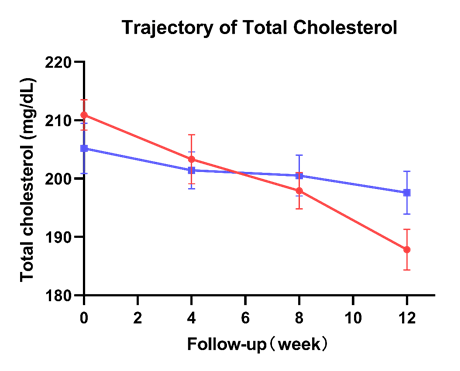
Figure 3: Mean change of total cholesterol. Note: (): Small molecule water group; (): Control group.
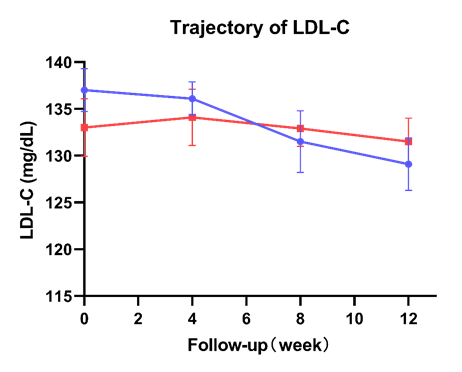
Figure 4: Mean change of LDL-C. Note: LDL-C: Low-Density Lipoprotein Cholesterol;(): Small molecule water group; (): Control group.
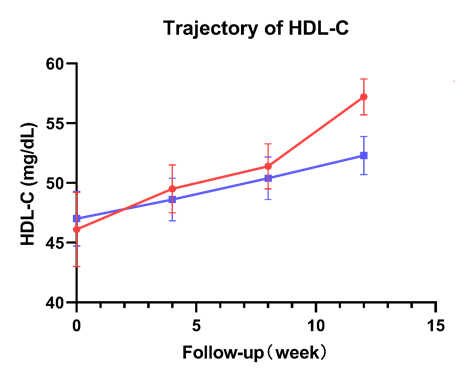
Figure 5: Mean change of HDL-C. Note: HDL-C: High-Density Lipoprotein Cholesterol; (): Small molecule water group; (): Control group.
The mean BMI decreased by 1.6 kg/m2 (95% CI 1.0-2.4 kg/m2) from baseline to 12 weeks in the intervention group and by 0.6kg/m2 (95% CI 0.2-1.1 kg/m2) in the control group, with a group difference of 1.0 kg/m2 (95% CI 0.4-1.8 kg/m2; p=0.016) (Figure 6).
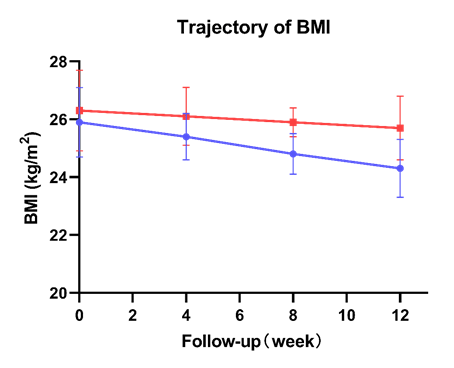
Figure 6: Mean change of BMI. Note: BMI: Body Mass Index; (): Small Molecule Water; (): Control group.
Safety
During follow-up, only one patient in the control group developed gout. There were no severe adverse events developed in the two groups.
DISCUSSION
In the randomized study with a three-month follow-up, we first found that SMW may reduce SUA in patients with asymptomatic hyperuricemia. The mean reductions in SUA were more significant in patients in the intervention group than those in the control group. Furthermore, SMW may also improve body metabolism in patients with asymptomatic hyperuricemia. The mean reductions in total cholesterol and LDL-C were more significant in patients in the intervention group than those in the control group. Also, the mean increase in HDL-C was more significant in patients in the intervention group compared with the control group. Our findings suggested that SMW may short termly improved body metabolism in these specific population.
Up to 21 % of the general population and 25% of hospitalized patients are estimated to have asymptomatic hyperuricemia, and uric acid levels can be elevated 10 to 15 years before clinical manifestations of gout [14,15]. The worldwide incidence of hyperuricemia is increasing in economically advantaged countries and the developing world as they adopt a Western diet and lifestyle [14,16]. Hyperuricemia is exceptionally high in Pacific islanders [17]. Men have higher rates than women, as estrogen is protective against hyperuricemia, and women can develop hyperuricemia after menopause [18,19]. In our trial, we found that females only accounted for 5.6% of all participants as the average age of this cohort was 30.5 ± 8.4 years old, and there are no sex differences in the definition of hyperuricemia in Chinese, so we did not perform subgroup analyses according to sex.
Hyperuricemia alone is not a specific indication for therapy (despite evidence linking it to the development of diabetes, hypertension, and cardiac disease). Most patients with elevated uric acid are asymptomatic and require no long-term therapy.
Hyperuricemia and hyperuricosuria have also been linked with other disorders such as metabolic syndrome, diabetes mellitus, cardiovascular disease, hypertension, atherosclerosis, obesity, and chronic renal disease [20-24]. In our previous studies, we found that asymptomatic hyperuricemia in elderly patients without comorbidities in Shanghai City was associated with a higher risk of incident congestive heart failure, stroke, and coronary artery disease, respectively [4-6]. Therefore, it is mandatory to explore an effective therapy to reduce serum uric acid in those with asymptomatic hyperuricemia.
Water intake is recognized to be essential for health maintenance and prevention of disease. However, the scientific evidence for this statement could be more substantial. There is no storage for water, and humans need to drink fluid several times daily. Water balance is achieved with varied individual intake depending on environmental temperature, physical activity, and kidney regulation. In addition to the amount of water, water composition should also be considered. A previous research group worked with natural mineral water rich in mineral salts and contains explicitly bicarbonate, chloride, sodium, and free carbon dioxide. They observed that consumption of one liter daily of this water for eight weeks as part of the usual diet reduced (LDL-C) and cardiovascular risk indexes (total cholesterol/ LDL-C and LDL-C /HDL-C) [25,26]. Also, the structure of water should be considered. Structured water is liquid water that is given an altered H-bonding structure by treatment with various forms of energy, including magnetic fields and light. SMW, characterized in the existing molecular structure of water, which is decomposed into single and stable water molecules, can directly permeate into all the cells and red blood cells of a human body to improve the absorption requirement of the cells of the human body to water molecules, and meet the water molecule and growth factor quantity required by all the cells of the human body to carry out metabolism in the human body [27]. The smaller the water cluster, the more water penetration, solvency, diffusion force, emulsifying power, metabolic force, and detergency will increase, water activation is more robust, and the oxygen content is higher [28]. A previous study reported that structured water may retard crystal formation, reduce urinary calcium and phosphorus excretion and promote earlier OPN mRNA expression in the rat kidney [10]. As we all know, no studies focused on the association between SMW and SUA or body metabolism in the clinical setting. In the present randomized study, we found that SMW short-termly improved body metabolism, including lowering SUA, total cholesterol, LDL-C, and BMI and increasing HDL-C. These parameters are significantly associated with adverse events such as morality, cardiovascular disease, or adverse fatal events. Thus, we dramatically wanted to know whether long-term consumption of SMW improved clinical prognosis in patients with metabolic syndrome.
Several limitations should be mentioned. Firstly, two-thirds of uric acid in the human body is excreted through the kidneys. So, drinking more water can help keep the pH value of urine at 6.3-6.8, which can make the uric acid easy to excrete and reduce the formation of uric acid crystals. In the current study, we did not measure urinary uric acid, electrolytes, or pH values. Thus, we needed to determine how SMW affects these parameters in the specific participants. Secondly, although each participant was instructed on a low-protein diet at the beginning of the study, we needed to monitor whether they effectively followed the low-protein diet during follow-up. However, the limitation may strengthen the results of small molecule water-reducing serum uric acid. Thirdly, due to the very short-term follow-up, we did not know whether small molecule water prevented gout, nephrolithiasis, or other adverse events. Lastly, all participants were from China, suggesting our findings may lack generalization to other ethnic populations.
CONCLUSION
In conclusion, we found that SMW may short-termly reduce serum uric acid and improve lipid metabolism in patients with asymptomatic hyperuricemia. Nonetheless, the long-term effects of SMW on SUA, gout, uric acid nephropathy, or cardiovascular disease remain unknown. Shortly, we will continuously conduct an RCT on the long-term effects of SMW on the adverse outcomes above in those with asymptomatic hyperuricemia.
AUTHOR CONTRIBUTIONS
Conceptualization, Xianfeng Wu and Wenhui He; methodology, Guihua Jian and Ruifeng Yang; software, Xiaojiang Zhan and Yueqiang Wen; validation, Na Tian and Fenfen Peng; formal analysis, Xianfeng Wu and Guihua Jian; Ivestigation, Fenfen Peng and Na Tian; resources, Xianfeng Wu, Yueqiang Wen, Xiaojiang Zhan, Na Tian, Junnan Wu, Ziran Peng, and Fenfen Peng; data curation, Guihua Jian and Xiaojiang Zhan; writing original draft preparation, Xianfeng Wu; writing review and editing, Xianfeng Wu; visualization, Ziran Peng and Niansong Wang; supervision, Niansong Wang and Wenhui He; project administration: Xianfeng Wu and Wenhui He. All authors have read and agreed to the published version of the manuscript.
ACKNOWLEDGEMENTS
This study received no funding. We express our gratitude to all patients who participated in the study.
COMPETING INTERESTS
All authors declare no financial or non-financial competing interests.
DATA AVAILABILITY
All data generated or analysed during this study are included in this published article.
CODE AVAILABILITY
Not applicable.
FUNDING INFORMATION
The study was supported by the Horizontal Project of Shanghai Sixth People's Hospital (Grant number: 2022-133).
REFRENCES
- Association SMDBoCNH. Multidisciplinary consensus expert group on the diagnosis and treatment of hyperuricemia-related diseases. Chin J Prac Int Med. 2023.
- Johnson RJ, Feig DI, Herrera-Acosta J, Kang DH. Resurrection of uric acid as a causal risk factor in essential hypertension. Hypertension. 2005;45(1):18-20.
[Google Scholar] [PubMed] [Crossref]
- Campion EW, Glynn RJ, Delabry LO. Asymptomatic hyperuricemia. Risks and consequences in the normative aging study. Am J Med. 1987;82(3):421-426.
[Google Scholar] [PubMed] [Crossref]
- Wu X, Jian G, Tang Y, Cheng H, Wang N, Wu J. Asymptomatic hyperuricemia and incident congestive heart failure in elderly patients without comorbidities. Nutr Metab Cardiovasc Dis. 2020;30(4):666-673.
[Google Scholar] [PubMed] [Crossref]
- Tu W, Wu J, Jian G, Lori J, Tang Y, Cheng H, et al. Asymptomatic hyperuricemia and incident stroke in elderly Chinese patients without comorbidities. Eur J Clin Nutr. 2019;73(10):1392-1402.
[Google Scholar] [PubMed] [Crossref]
- Wu J, Lei G, Wang X, Tang Y, Cheng H, Jian G, et al. Asymptomatic hyperuricemia and coronary artery disease in elderly patients without comorbidities. Oncotarget. 2017;8(46):80688.
[Google Scholar] [PubMed] [Crossref]
- Kuwabara M, Niwa K, Hisatome I, Nakagawa T, Roncal-Jimenez CA, Andres-Hernando A, et al. Asymptomatic hyperuricemia without comorbidities predicts cardiometabolic diseases: Five-year Japanese cohort study. Hypertension. 2017;69(6):1036-1044.
[Google Scholar] [PubMed] [Crossref]
- Shultz MJ, Vu TH, Meyer B, Bisson P. Water: A responsive small molecule. Acc Chem Res. 2012;45(1):15-22.
[Google Scholar] [PubMed] [Crossref]
- Keutsch FN, Saykally RJ. Water clusters: Untangling the mysteries of the liquid, one molecule at a time. Proc Natl Acad Sci U S A. 2001;98(19):10533-1040.
[Google Scholar] [PubMed] [Crossref]
- Li Y, Pan J, Zhang Y, Chang Y, Yang X, Yang B, et al. Effects of small molecules water that may retard kidney stone formation. Int Urol Nephrol. 2018;50(2):225-230.
[Google Scholar] [PubMed] [Crossref]
- Kalantar-Zadeh K, Joshi S, Schlueter R, Cooke J, Brown-Tortorici A, Donnelly M, et al. Plant-dominant low-protein diet for conservative management of chronic kidney disease. Nutrients. 2020;12(7):1931.
[Google Scholar] [PubMed] [Crossref]
- Senn S. Change from baseline and analysis of covariance revisited. Stat Med. 2006;25(24):4334-4344.
[Google Scholar] [PubMed] [Crossref]
- Sterne JA, White IR, Carlin JB, Spratt M, Royston P, Kenward MG, et al. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. Bmj. 2009;338.
[Google Scholar] [PubMed] [Crossref]
- Li L, Zhang Y, Zeng C. Update on the epidemiology, genetics, and therapeutic options of hyperuricemia. Am J Transl Res. 2020;12(7):3167.
[Google Scholar] [PubMed]
- Williams LA. The history, symptoms, causes, risk factors, types, diagnosis, treatments, and prevention of gout, part 2. Int J Pharm Compd. 2019;23(1):14-21.
[Google Scholar] [PubMed]
- Singh G, Lingala B, Mithal A. Gout and hyperuricaemia in the USA: Prevalence and trends. Rheumatology. 2019;58(12):2177-2180.
[Google Scholar] [PubMed]
- Gosling AL, Matisoo-Smith E, Merriman TR. Hyperuricaemia in the Pacific: Why the elevated serum urate levels?. Rheumatol Int. 2014;34(6):743-757.
[Google Scholar] [PubMed] [Crossref]
- Wu X, You C. The biomarkers discovery of hyperuricemia and gout: Proteomics and metabolomics. PeerJ. 2023;11:e14554.
[Google Scholar] [PubMed] [Crossref]
- Yokokawa H, Fukuda H, Suzuki A, Fujibayashi K, Naito T, Uehara Y, Nakayama A, Matsuo H, Sanada et al. Association between serum uric acid levels/hyperuricemia and hypertension among 85,286 Japanese workers. J Clin Hypertens. 2016;18(1):53-59.
[Google Scholar] [PubMed] [Crossref]
- Barkas F, Elisaf M, Liberopoulos E, Kalaitzidis R, Liamis G. Uric acid and incident chronic kidney disease in dyslipidemic individuals. Curr Med Res Opin. 2018;34(7):1193-1199.
[Google Scholar] [PubMed] [Crossref]
- Song D, Zhao X, Wang F, Wang G. A brief review of Urate Transporter 1 (URAT1) inhibitors for the treatment of hyperuricemia and gout: Current therapeutic options and potential applications. Eur J Pharmacol. 2021;907:174291.
[Google Scholar] [PubMed] [Crossref]
- Bhole V, Choi JW, Kim SW, De Vera M, Choi H. Serum uric acid levels and the risk of type 2 diabetes: A prospective study. Am J Med. 2010;123(10):957-961.
[Google Scholar] [PubMed] [Crossref]
- Borghi C, Rosei EA, Bardin T, Dawson J, Dominiczak A, Kielstein JT, et al. Serum uric acid and the risk of cardiovascular and renal disease. J Hypertens. 2015;33(9):1729-1741.
[Google Scholar] [PubMed] [Crossref]
- Borghi C. The role of uric acid in the development of cardiovascular disease. Curr Med Res Opin. 2015;31(sup2):1-2.
[Google Scholar] [PubMed] [Crossref]
- Schoppen S, Perez-Granados AM, Vaquero MP, Carbajal Á, Oubiña P, Sánchez-Muniz FJ, et al. A sodium-rich carbonated mineral water reduces cardiovascular risk in postmenopausal women. J Nutr. 2004;134(5):1058-1063.
[Google Scholar] [PubMed] [Crossref]
- Pérez-Granados AM, Navas-Carretero S, Schoppen S, Vaquero MP. Reduction in cardiovascular risk by sodium-bicarbonated mineral water in moderately hypercholesterolemic young adults. J Nutr Biochem. 2010;21(10):948-953.
[Google Scholar] [PubMed] [Crossref]
- Small molecule water and its prepn process and preparing activator.
- Guidelines for drinking‑water quality.
Author(s) Info
1 Department of Nephrology, Shanghai Jiao Tong University Affiliated Sixth People's Hospital, Shanghai, China2 Department of Nephrology, The First Affiliated Hospital of Nanchang University, Nanchang, China
3 Department of Nephrology, The Second Affiliated Hospital of Guangzhou Medical University, Guangzhou, China
4 Department of Nephrology, Shanghai Ocean University, Shanghai, China
5 Department of Nephrology, Zhujiang Hospital of Southern Medical University, Guangzhou, China
6 Department of Nephrology, Zhejiang University Medical College Affiliated Sir Run Run Shaw Hospital, Hangzhou, China
7 Department of Nephrology, General Hospital of Ningxia Medical University, Yinchuan, China
8 Department of Nephrology, Shanghai Ocean University, Shanghai, China
Received date: 22-Aug-2025, Manuscript No: JNP-25-165628; Accepted date: 08-Sep-2025 Published date: 10-Oct-2025
Citation: Wu X, Jian G, Yang R, Zhan X, Wen Y, Peng Z, et al. (2025) Efficacy and Safety of Small Molecule Water in Patients with Asymptomatic Hyperuricemia: A Multicenter, Randomized, Double-blind, Placebo-controlled Trial. J Nephrol.1: 001.
Copyright: © 2025 Wu X, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
