Clinical features and outcomes of symptomatic urinary stone disease: An analysis according to stone compositions
Abstract
Background: The incidence of urinary stone disease is increasing, and these patients are at greater risk for various kidney complications. Given its heterogeneity and potential clinical implications, we investigated the baseline characteristics and clinical outcomes of symptomatic stone disease according to stone compositions.
Methods: This was a single-center, retrospective study that analysed symptomatic urinary stone disease patients with known stone compositions from 2002 to 2020. Patients were grouped into three categories: calcium-containing, urate, and struvite stones. Baseline characteristics, prevalence of diverse comorbidities, concurrent acute kidney injury (AKI) events, long-term kidney function deterioration, and mortality were analysed.
Results: Calcium-containing stones were the most common type. Patients with urate stones were significantly older, predominantly male, and more likely to have various comorbidities and low urinary pH. Calcium excretion was significantly higher in patients with calcium-containing stones, while the excretion of other components was comparable across all stone compositions. The incidence of AKI in symptomatic urinary stone disease patients was 35.3%. Of note, urate and struvite stones were independently associated with concurrent AKI. An eGFR decline of more than 30% was observed in 5.7% of the patients, with the highest rates among patients with urate stones. Older age, female sex, higher baseline serum creatinine level, and concurrent AKI episodes, but not stone composition, were independently associated with subsequent kidney function deterioration.
Conclusion: In symptomatic urinary stone disease, concurrent AKI episodes, older age, female sex, and lower baseline kidney function were independently associated with progressive kidney function deterioration, regardless of stone composition.
Urinary stone disease; Stone composition; Risk factors; Acute kidney injury; Kidney function deterioration
ABBREVATIONS
Acute Kidney Injury (AKI); Chronic Kidney Disease (CKD); Chronic Obstructive Pulmonary Disease (COPD); C-Reactive Protein (CRP); estimated Glomerular Filtration Rate (eGFR); End-Stage Kidney Disease (ESKD); Erythrocyte Sedimentation Rate (ESR); Extracorporeal Shock Wave Lithotripsy (ESWL); Hazard Ratio (HR); Institutional Review Board (IRB); National Health Insurance Service (NHIS); National Kidney Foundation and the U.S. Food and Drug Administration (NKF-FDA); Non-Steroidal Anti-Inflammatory Drugs (NSAIDs); Odds Ratio (OR)
INTRODUCTION
Several epidemiological studies have shown that the incidence of urinary stone diseases is increasing. Although its incidence varies depending on the geological, clinical, and social characteristics, it is undeniable that it is emerging as a global concern. In the United States, one in 11 individuals experience kidney stone disease during their lifetime [1]. A study conducted on 1,543 adults in Florence, Italy, reported a prevalence of 7.5%, and a recurrence rate of more than 50% [2]. In Asian countries, the reported incidence is somewhat lower, but an increasing trend in urinary stone disease with its associated social burden is also noted. Zeng et al. reported that the prevalence of kidney stones in China was 6.4% [3]. A recent study from South Korea that analysed the National Health Insurance Service (NHIS) sample cohort dataset showed that the annual incidence of urinary stone disease is 3.27 per 1,000 person-years [4]. Despite limitations in direct comparison due to differences in patient populations and methods used for analysis, it is evident that urinary stone disease is emerging as an increasingly important global medical issue.
Traditionally, urinary stone disease is considered a urologic disorder, requiring pain management and stone removal. However, recent nephrological perspectives reported that it is more chronic medical conditions that are associated with acute kidney injury (AKI), chronic kidney disease (CKD), end stage kidney disease (ESKD) and other metabolic diseases, contributing to an increase in morbidity and mortality [5-10].
Until recently, most studies have been population-based historical cohort studies that used diagnostic codes without considering the stone types. Considering that urinary stone disease is a highly heterogeneous condition with different risk factors and concurrent comorbidities that are potentially linked to different clinical outcomes according to stone composition [11], we analysed symptomatic patients with stones of known composition. Baseline characteristics, including comorbid conditions, urinalysis, and 24-hour urine chemistry, as well as risk factors for concurrent AKI, subsequent kidney function deterioration, and mortality were analysed [12].
MATERIALS AND METHODS
Study population and data selection
This single-center, retrospective observational study analysed data from patients admitted to the Department of Nephrology or Urology, Korea University Anam Hospital, due to symptomatic urinary stone disease, between January 2002 and December 2020. All included patients had baseline serum creatinine measurements. This study was approved by the Institutional Review Board (IRB) of the Korea University Anam Hospital (IRB approval No. 2022AN0310). We included all patients whose stone composition was analysed using ureteroscopic removal or ESWL (extracorporeal shock wave lithotripsy) during the study. Demographic and laboratory data, including blood biochemistry, urinalysis, and 24-hour urine chemistry, were collected. Concurrent AKI and long-term outcome data regarding kidney function deterioration and mortality were analysed. Moreover, 24-hour urine chemistry, from 233 patients were also analysed.
Stone classification
Stone composition was analysed using Fourier transform infrared spectroscopy. The stone analysis test items were structured to list the presence or absence of individual components, such as calcium, oxalate, and urate. The stone composition groups were redefined based on, the classification established by the Mayo Clinic [13]. Stones were classified as follows: 1) stones containing phosphate, ammonium, or magnesium were classified as struvite stones; 2) stones containing urate were classified as urate stones; 3) stones containing calcium or oxalate were classified as calcium-containing stones. Patients with mixed stones of more than two main component types (e.g. stones containing both calcium and urate) and those with unclassified stones were excluded from the analysis. Subsequently, 725 patients were classified into three groups based on stone composition as follows: 1) calcium-containing stones; 2) urate stones; and, 3) struvite stones. Patients with brushite and cystine stones were not identified in the study population.
Definition
The baseline serum creatinine level was defined as the average of all serum creatinine values measured in the year immediately preceding the year of admission for stone removal. AKI was defined as a rise of serum creatinine ≥ 0.3mg/dL compared with baseline serum creatinine, or the need for temporary dialysis treatment, at the time of treatment for urinary stone disease. The estimated glomerular filtration rate (eGFR) was obtained from serum creatinine levels using the 2021 version of the CKD-EPI (chronic kidney disease epidemiology collaboration) equation. CKD was defined as baseline eGFR <60 ml/min/1.73m2, based on the baseline creatinine level. Patients were defined as having ESKD progression if they required maintenance hemodialysis, peritoneal dialysis, or kidney transplantation. Kidney function deterioration was defined as a comprehensive concept, indicating a decline of more than 30% in eGFR calculated by comparing the baseline eGFR and eGFR estimated from the last serum creatinine measurement during the study period or progression to ESKD. This threshold was supported as a surrogate endpoint for progressive CKD in large-scale meta-analysis and expert consensus, including the NKF-FDA (National Kidney Foundation and the U.S. Food and Drug Administration) workshop report and subsequent validation in clinical outcome studies [14,15].
The data collected from the patient charts included demographics, comorbidities, stone analysis, blood tests, and urine extractions. The baseline patient characteristics were collected at the time of first admission. Data regarding progression to ESKD and mortality were collected from the registry of the Korean Society of Nephrology and the National Database of Statistics, Korea, and electronic medical records, respectively.
Statistical Analysis
Categorical variables were reported as frequencies and percentages, and continuous variables were reported as means and standard deviations. The stone composition groups were compared using one-way analysis of variance with Tukey’s post hoc analysis. A subgroup analysis was performed for patients who completed 24-hour urine collection, and a complete case analysis was applied by excluding those with missing data.
Multivariate logistic regression analysis was performed to identify and assess risk factors for AKI. Results were expressed as odds ratios (ORs) with corresponding 95% confidence intervals. Cox proportional hazards model was used for risk factors for mortality and kidney function deterioration. Results were reported as hazard ratios (HRs) with 95% confidence intervals. For logistic regression and Cox analyses, variables were chosen using p<0.05 in univariate analysis, along with age and sex. Statistical significance was set at p<0.05 was considered significant. All analyses were performed using the SPSS software (SPSS version 23.0, Chicago, IL, USA).
RESULTS
Study participants
Among the 758 patients admitted for symptomatic urinary stone disease who underwent stone removal procedures during the study period, a total of 33 patients were excluded: 30 with mixed or unclassified stones and 3 with a history of ESKD. Finally, 725 patients were included. The mean age of the participants was 58.7 years, with 64.3% being male (N=466). Twenty-four urine samples were collected from the 233 patients.
Baseline demographics and laboratory data according to stone subtypes
Table 1 shows the baseline demographic and laboratory data. Calcium-containing stones were the most common subtype (N=510, 70.3%), followed by struvite (N=117, 16.1%) and urate stones (N=98, 13.5%). Patients with urate stones were significantly older, were predominantly male, and had a higher prevalence of comorbidities including diabetes, hypertension, heart failure, dementia, chronic obstructive pulmonary disease (COPD), cancer, and CKD. The differences in baseline laboratory data according to the stone subtype were also remarkable. Those with urate stones had significantly lower hemoglobin and total cholesterol levels, higher uric acid levels, and lower eGFR than those with the other stone subtypes. Patients with struvite stones were characterized by lower total CO2 , phosphate, and albumin levels, while inflammatory markers such as c-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) were significantly elevated, suggesting the presence of concurrent urinary tract infections.
| Characteristics | Ca containing stone (n=510, 70.3%) | Urate stone (n=98, 13.5%) | Struvite stone (n=117, 16.1%) | p-value |
|---|---|---|---|---|
| Sex, male, n (%) | 322 (63.1%) | 75 (76.5%)* | 69 (59.0%)% | 0.017 |
| Age (years) | 57.44 ± 13.41 | 67.95 ± 12.94* | 56.38 ± 15.89% | <0.001 |
| BMI (kg/m2) | 24.94 ± 3.74 | 25.25 ± 3.60 | 26.54 ± 26.96 | 0.388 |
| Comorbidities | ||||
| DM, n (%) | 140 (27.5%) | 47 (48.0%)* | 22 (18.8%)% | <0.001 |
| HTN, n (%) | 230 (45.1%) | 71 (72.4%)* | 53 (45.3%)%$ | <0.001 |
| Chronic liver disease,n (%) | 69 (13.5%) | 12 (12.2%) | 14 (12.0%) | 0.870 |
| IHD, n (%) | 37 (7.3%) | 14 (14.3%) | 11 (9.4%) | 0.070 |
| PAOD, n (%) | 23 (4.5%) | 9 (9.2%) | 4 (3.4%) | 0.105 |
| HF, n (%) | 6 (1.2%) | 6 (6.1%)* | 4 (3.4%) | 0.006 |
| Dementia, n (%) | 5 (1.0%) | 4 (4.1%)* | 1 (0.9%) | 0.047 |
| Hemiparesis, n (%) | 6 (1.2%) | 1 (1.0%) | 2 (1.7%) | 0.876 |
| COPD, n (%) | 8 (1.6%) | 9 (9.2%)* | 4 (3.4%)% | <0.001 |
| Cancer, n (%) | 71 (13.9%) | 24 (24.5%)* | 22 (18.8%) | 0.023 |
| CKD, n (%) | 25 (4.9%) | 42 (42.9%)* | 8 (6.8%)% | <0.001 |
| Laboratory test | ||||
| Hb (g/dL) | 14.11 ± 1.68 | 13.52 ± 2.11* | 13.74 ± 2.12 | 0.004 |
| WBC ( × 103/µL) | 8.17 ± 3.47 | 8.80 ± 4.51 | 8.34 ± 3.72 | 0.299 |
| Na (mmol/L) | 139.54 ± 2.81 | 138.99 ± 3.14 | 139.44 ± 3.18 | 0.234 |
| K (mmol/L) | 4.16 ± 0.39 | 4.27 ± 0.46* | 4.12 ± 0.43% | 0.019 |
| Cl (mmol/L) | 104.11 ± 2.91 | 103.68 ± 3.38 | 104.25 ± 3.35 | 0.359 |
| Total CO2 (mmol/L) | 25.27 ± 3.26 | 24.44 ± 3.62 | 24.11 ± 3.59$ | 0.012 |
| BUN (mg/dL) | 16.06 ± 7.69 | 21.59 ± 11.89* | 16.99 ± 10.00% | <0.001 |
| Baseline Cr (mg/dL) | 0.87 ± 0.31 | 1.15 ± 0.31* | 0.88 ± 0.45% | <0.001 |
| Baseline eGFR (mL/min/1.73m2) | 89.67 ± 16.91 | 65.93 ± 19.61* | 90.66 ± 20.95% | <0.001 |
| Total Ca (mg/dL) | 9.21 ± 0.68 | 9.15 ± 0.70 | 9.30 ± 0.93 | 0.380 |
| Phosphate (mg/dL) | 3.52 ± 0.63 | 3.42 ± 0.66 | 3.23 ± 0.87$ | 0.002 |
| Magnesium (mmol/L) | 0.85 ± 0.09 | 0.85 ± 0.11 | 0.85 ± 0.11 | 0.960 |
| Uric acid (mg/dL) | 5.55 ± 1.65 | 6.19 ± 1.69* | 5.66 ± 2.02 | 0.012 |
| Protein (g/dL) | 7.16 ± 0.57 | 7.12 ± 0.58 | 7.07 ± 0.68 | 0.304 |
| Albumin (g/dL) | 4.32 ± 0.44 | 4.22 ± 0.44 | 4.20 ± 0.57$ | 0.011 |
| CRP (mg/L) | 20.29 ± 50.35 | 27.22 ± 65.54 | 41.11 ± 75.61$ | 0.008 |
| ESR (mm/hr) | 19.06 ± 19.97 | 28.59 ± 30.38* | 28.75 ± 31.07$ | <0.001 |
| Glucose (mg/dL) | 125.62 ± 47.32 | 131.72 ± 43.84 | 117.85 ± 51.78 | 0.098 |
| Total cholesterol (mg/dL) | 185.17 ± 43.08 | 169.60 ± 38.86* | 182.29 ± 46.43 | 0.005 |
| LDL cholesterol (mg/dL) | 111.38 ± 35.68 | 105.91 ± 36.36 | 116.79 ± 35.03 | 0.217 |
| HDL cholesterol (mg/dL) | 45.52 ± 11.95 | 43.81 ± 12.16 | 46.53 ± 12.01 | 0.428 |
| Triglyceride (mg/dL) | 153.49 ± 88.20 | 155.33 ± 101.97 | 145.72 ± 96.59 | 0.781 |
| Note: Data are presented as numbers (percentage) or mean ± standard deviation. BMI: Body Mass Index; DM: Diabetes Mellitus; HTN: Hypertension; IHD: Ischemic Heart Disease; PAOD: Peripheral Arterial Disease; HF: Heart Failure; COPD: Chronic Obstructive Pulmonary Disease; CKD: Chronic Kidney Disease; Hb: Hemoglobin; WBC: White Blood Cell; Na: Sodium; K: Potassium; Cl: Chloride; BUN: Blood urea nitrogen; Cr: Creatinine; eGFR: estimated Glomerular Filtration Rate; Total Ca: Total Calcium; CRP: C-Reactive Protein; ESR: Erythrocyte Sedimentation Rate; LDL: Low-Density Lipoprotein; HDL: High-Density Lipoprotein. Stone composition groups were compared using one-way analysis of variance with Tukey post-hoc analysis. A p value ≤ 0.050 was considered as statistically significant. *Ca Containing stone vs. Urate stone, $Ca Containing stone vs. Struvite stone, %Urate stone vs. Struvite stone (post-hoc analysis) | ||||
Table 1: Baseline demographics, clinical characteristics, and laboratory findings according to stone subtypes.
Urinary parameters according to stone subtypes
Urine pH was significantly low in patients with urate stones, while those with struvite stones had a higher urine pH (Table 2). Urine biochemistry using 24-hour urine collection data was available only in 233 patients (32.1%). The analysis showed that calcium excretion was significantly elevated in patients with calcium-containing stones. However, the excretion of sodium, uric acid, citrate, oxalate, and protein did not vary according to different stone compositions (Table 2). However, the high missing rate of the 24-hour urine study might affect the results of the analysis.
| Urinary excretory variables, Mean ± SD | Ca containing stone (n=513, 70.5%) | Urate stone (n=98, 13.5%) | Struvite stone (n=117, 16.1%) | p-value |
|---|---|---|---|---|
| Urine SG | 1.01 ± 0.006 | 1.01 ± 0.006 | 1.01 ± 0.006 | 0.772 |
| Urine pH | 6.09 ± 0.89 | 5.59 ± 0.84* | 6.40 ± 0.98$% | <0.001 |
| 24-hr urine variable,Mean ± SD | Ca containing stone (n=139, 59.7%) | Urate stone (n=53, 22.7%) | Struvite stone (n=117, 17.6%) | p-value |
| Sodium (mmol/d) | 178.43 ± 89.40 | 186.13 ± 115.96 | 150.93 ± 109.56 | 0.350 |
| Potassium (mmol/d) | 54.10 ± 25.08 | 55.02 ± 38.33 | 44.81 ± 24.04 | 0.290 |
| Chloride (mmol/d) | 192.39 ± 94.72 | 194.14 ± 116.91 | 162.93 ± 108.38 | 0.391 |
| Total calcium (mg/d) | 193.22 ± 139.25 | 74.84 ± 60.81* | 163.59 ± 136.96% | 0.000 |
| Phosphate (mg/d) | 594.66 ± 340.89 | 573.62 ± 302.88 | 426.48 ± 244.57 | 0.121 |
| Magnesium (mmol/d) | 3.77 ± 1.83 | 4.60 ± 2.61 | 3.34 ± 2.08 | 0.154 |
| Uric acid (mg/d) | 560.73 ± 269.95 | 594.04 ± 341.70 | 493.38 ± 272.26 | 0.395 |
| Protein (mg/d) | 438.40 ± 1493.28 | 531.87 ± 1264.74 | 528.80 ± 990.02 | 0.905 |
| Citrate (mg/d) | 218.49 ± 235.44 | 119.29 ± 134.11 | 182.41 ± 187.34 | 0.165 |
| Oxalate (mg/d) | 27.88 ± 13.33 | 30.77 ± 13.28 | 25.87 ± 13.30 | 0.476 |
| Note: Data are presented as mean ± standard deviation. urine SG, urine specific gravity. Stone composition groups were compared using one-way analysis of variance with Tukey post-hoc analysis. A p value ≤ 0.050 was considered as statistically significant. *Ca Containing stone vs. Urate stone, $Ca containing stone vs. Struvite stone, %Urate stone vs. Struvite stone (post-hoc analysis) | ||||
Table 2: Random urine findings and 24-hour urinary excretory parameters according to stone subtypes.
AKI according to stone composition
Among the 725 patients, 256 (35.3%) had concurrent AKI. The incidence of AKI was highest in those with urate stones (63.3%), followed by those with struvite (39.3%) and calcium (29%) stones (Table 3).
| Subtypes | Ca containing stone | Urate stone | Struvite stone | p-value |
|---|---|---|---|---|
| Acute kidney injury | 148 (29.0%) | 62 (63.3%)* | 46 (39.3%)% | <0.001 |
| Stage 1 | 122 (23.9%) | 40 (40.8%) | 36 (30.8%) | |
| Stage 2 | 19 (3.7%) | 10 (10.2%) | 4 (3.4%) | |
| Stage 3 | 7 (1.4%) | 12 (12.2%) | 6 (5.1%) | |
| Note: Stone composition groups were compared using one-way analysis of variance with Tukey post-hoc analysis. A p value ≤ 0.050 was considered as statistically significant. *Ca Containing stone vs. Urate stone, $Ca Containing stone vs. Struvite stone, %Urate stone vs. Struvite stone (post-hoc analysis) | ||||
Table 3: Incidence of acute kidney injury according to stone subtypes.
Patients with AKI were more likely to be older and to have other comorbidities, such as diabetes, hypertension, chronic liver disease, hemiparesis, COPD, cancer, and CKD than those without AKI. Patients with concurrent AKI showed significantly lower hemoglobin, serum total CO2 , total calcium, protein, and albumin levels than those without AKI. Concurrent AKI was also associated with higher leukocyte counts and higher CRP, ESR, and uric acid levels (Table 4).
| Characteristics | No AKI (n=469, 64.7%) | AKI (n=256, 35.3%) | Total (n=725) | p-value |
|---|---|---|---|---|
| Sex, male, n (%) | 301 (64.2%) | 165 (64.5%) | 466 (64.3%) | 1.000 |
| Age (years) | 57.07 ± 14.17 | 61.64 ± 13.94 | 58.69 ± 14.25 | <0.001 |
| BMI | 24.79 ± 3.65 | 26.01 ± 17.84 | 25.22 ± 10.98 | 0.285 |
| Comorbidities | ||||
| DM, n (%) | 109 (23.2%) | 100 (39.1%) | 209 (28.8%) | <0.001 |
| HTN, n (%) | 196 (41.8%) | 158 (61.7%) | 354 (48.8%) | <0.001 |
| Chronic liver disease,n (%) | 52 (11.1%) | 43 (16.8%) | 95 (13.1%) | 0.038 |
| IHD, n (%) | 35 (7.5%) | 27 (10.5%) | 62 (8.6%) | 0.166 |
| PAOD, n (%) | 21 (4.5%) | 15 (5.9%) | 36 (5.0%) | 0.475 |
| HF, n (%) | 7 (1.5%) | 9 (3.5%) | 16 (2.2%) | 0.110 |
| Dementia, n (%) | 6 (1.3%) | 4 (1.6%) | 10 (1.4%) | 0.748 |
| Hemiparesis, n (%) | 2 (0.4%) | 7 (2.7%) | 9 (1.2%) | 0.011 |
| COPD, n (%) | 8 (1.7%) | 13 (5.1%) | 21 (2.9%) | 0.018 |
| Cancer, n (%) | 61 (13.0%) | 56 (21.9%) | 117 (16.1%) | 0.003 |
| CKD, n (%) | 18 (3.8%) | 57 (22.3%) | 75 (10.3%) | <0.001 |
| Laboratory test | ||||
| Hb (g/dL) | 14.25 ± 1.63 | 13.46 ± 2.05 | 13.97 ± 1.83 | <0.001 |
| WBC (× 103 /µL) | 7.95 ± 3.16 | 8.89 ± 4.40 | 8.28 ± 3.67 | 0.003 |
| Na (mmol/L) | 139.58 ± 2.53 | 139.20 ± 3.52 | 139.45 ± 2.92 | 0.123 |
| K (mmol/L) | 4.17 ± 0.38 | 4.17 ± 0.46 | 4.17 ± 0.41 | 0.989 |
| Cl (mmol/L) | 104.12 ± 2.74 | 103.98 ± 3.56 | 104.07 ± 3.05 | 0.592 |
| Total CO2 (mmol/L) | 25.50 ± 3.07 | 24.12 ± 3.68 | 24.89 ± 3.42 | <0.001 |
| BUN (mg/dL) | 15.29 ± 4.89 | 20.01 ± 13.00 | 16.96 ± 8.95 | <0.001 |
| Baseline Cr (mg/dL) | 0.84 ± 0.19 | 1.05 ± 0.50 | 0.91 ± 0.35 | <0.001 |
| Baseline eGFR (mL/min/1.73m2) | 91.80 ± 15.40 | 77.13 ± 23.07 | 86.62 ± 19.75 | <0.001 |
| Total Ca (mg/dL) | 9.27 ± 0.62 | 9.13 ± 0.87 | 9.22 ± 0.73 | 0.040 |
| Phosphate (mg/dL) | 3.49 ± 0.65 | 3.42 ± 0.74 | 3.46 ± 0.69 | 0.289 |
| Magnesium (mmol/L) | 0.85 ± 0.08 | 0.85 ± 0.10 | 0.85 ± 0.09 | 0.357 |
| Uric acid (mg/dL) | 5.42 ± 1.48 | 6.04 ± 2.01 | 5.67 ± 1.73 | <0.001 |
| Protein (g/dL) | 7.19 ± 0.51 | 7.04 ± 0.70 | 7.14 ± 0.59 | 0.002 |
| Albumin (g/dL) | 4.36 ± 0.39 | 4.14 ± 0.55 | 4.29 ± 0.47 | <0.001 |
| CRP (mg/L) | 17.23 ± 43.66 | 36.15 ± 73.25 | 24.69 ± 57.88 | 0.001 |
| ESR (mm/hr) | 16.89 ± 18.13 | 30.17 ± 29.93 | 22.37 ± 24.58 | <0.001 |
| Glucose (mg/dL) | 122.45 ± 42.46 | 130.21 ± 55.81 | 125.19 ± 47.71 | 0.053 |
| Total cholesterol (mg/dL) | 186.95 ± 41.58 | 174.58 ± 45.45 | 182.59 ± 43.36 | <0.001 |
| LDL cholesterol (mg/dL) | 114.39 ± 33.91 | 106.29 ± 38.18 | 111.37 ± 35.73 | 0.031 |
| HDL cholesterol (mg/dL) | 46.04 ± 11.86 | 44.30 ± 12.17 | 45.41 ± 11.99 | 0.159 |
| Triglyceride (mg/dL) | 146.73 ± 94.21 | 162.39 ± 86.58 | 152.53 ± 91.67 | 0.075 |
| Urine test | ||||
| Urine SG | 1.02 ± 0.01 | 1.01 ± 0.01 | 1.01 ± 0.01 | 0.159 |
| Urine pH | 6.10 ± 0.92 | 6.02 ± 0.94 | 6.07 ± 0.93 | 0.290 |
| Note: Data are presented as numbers (percentage) or mean ± standard deviation. AKI: Acute Kidney Injury; BMI: Body Mass Index; DM: Diabetes Mellitus; HTN: Hypertension; IHD: Ischemic Heart Disease; PAOD: Peripheral Arterial Disease; HF: Heart Failure; COPD: Chronic Obstructive Pulmonary Disease; CKD: Chronic Kidney Disease; Hb: Hemoglobin; WBC: White Blood Cell; Na: Sodium; K: Potassium; Cl: Chloride; BUN: Blood Urea Nitrogen; Cr: Creatinine; eGFR: estimated Glomerular Filtration Rate; Total Ca: Total Calcium; CRP: C-Reactive Protein; ESR: Erythrocyte Sedimentation Rate; LDL: Low-Density Lipoprotein; HDL: High-Density Lipoprotein. Comparison between AKI vs. non- AKI groups were done using Student’s t-test (continuous variables) or Chi-square test (categorical variables). A p value ≤ 0.05 was considered as statistically significant. | ||||
Table 4: Baseline demographics, clinical characteristics, laboratory findings, and random urinary findings by acute kidney injury status.
In the multivariate logistic regression analysis, patients with urate stones had a 98.4% higher risk of developing AKI event (OR 1.984, 95% Confidence Interval [CI] 1.047-3.761, p=0.036) than those with calcium-containing stones. Patients with struvite stones also showed a 92.7% higher risk of AKI events (OR 1.927, 95% CI 1.119-3.317, p=0.018) than those with calcium containing stones, indicating that stone composition was an independent risk factor for AKI. Additionally, hypertension (OR 1.968, 95% CI 1.233-3.142, p=0.005), high baseline serum creatinine levels (OR 19.255, 95% CI 4.225-87.765, p<0.001), high uric acid levels (OR 1.224, 95% CI 1.062-1.410, p=0.005), low hemoglobin (OR 0.827, 95% CI 0.715-0.957, p=0.011), and low serum albumin levels (OR 0.436, 95% CI 0.273-0.696, p=0.001) were also found to be independent risk factors of concurrent AKI in symptomatic urinary stone disease patients (Table 5).
| For AKI | Odds ratio | 95% CI | p-value |
|---|---|---|---|
| Sex (Female to male) | 1.604 | 0.912-2.823 | 0.101 |
| Age, years | 0.999 | 0.982-1.016 | 0.881 |
| DM | 1.369 | 0.871-2.152 | 0.173 |
| HTN | 2.005 | 1.258-3.196 | 0.003 |
| Baseline Cr (mg/dL) | 12.532 | 4.006-39.204 | <0.001 |
| Hb (g/dL) | 0.828 | 0.715-0.958 | 0.011 |
| Uric acid (mg/dL) | 1.224 | 1.063-1.411 | 0.005 |
| Albumin (g/dL) | 0.442 | 0.277-0.706 | 0.001 |
| Stone composition (based on calcium containing stone) | - | - | 0.017 |
| Urate stone | 1.911 | 1.014-3.600 | 0.045 |
| Struvite stone | 1.889 | 1.101-3.241 | 0.021 |
| Note: CI: confidence interval; DM: diabetes mellitus; HTN: hypertension; Cr: creatinine; Hb: hemoglobin. | |||
Table 5: Logistic regression analysis of factors associated with acute kidney injury.
Mortality and kidney function deterioration according to stone composition
During the mean follow-up of 852.2 days, 33 patients (4.6%) died and 42 patients (5.8%) showed kidney function deterioration defined as an eGFR decrease of more than 30% from baseline or ESKD progression. Patients with urate stones had significantly higher rates of both mortality and kidney function deterioration (Table 6).
| Ca containing stone (n=510, 70.3%) | Urate stone (n=98, 13.5%) | Struvite stone (n=117, 16.1%) | p-value | |
|---|---|---|---|---|
| Mortality | 14 (2.7%) | 11 (11.2%)* | 8 (6.8%) | 0.001 |
| Kidney function deterioration | 22 (4.3%) | 12 (12.2%)* | 8 (6.8%) | 0.008 |
| Note: Stone composition groups were compared using one-way analysis of variance with Tukey post-hoc analysis. A p value ≤ 0.050 was considered as statistically significant. *Ca Containing stone vs. Urate stone, $Ca Containing stone vs. Struvite stone, %Urate stone vs. Struvite stone (post-hoc analysis) | ||||
Table 6: Incidence of mortality and kidney function deterioration according to stone subtypes.
No independent risk factors for mortality were identified in the Cox proportional hazards model analysis (Table 7). In contrast, concurrent AKI episodes (HR 7.887, 95% CI 2.719-22.880, p<0.001), older age (HR=1.047, 95% CI 1.016-1.078, p=0.002), female sex (HR 1.992, 95% CI 1.032-3.845, p=0.040), and high baseline serum creatinine (HR 2.103, 95% CI 1.477 2.995, p<0.001) were independent predictors of kidney function deterioration (Table 8, Figure 1). Notably, stone composition was not an independent factor for subsequent kidney function deterioration.
| For mortality | Hazard ratio | 95% CI | p-value |
|---|---|---|---|
| Sex (Female to male) | 1.965 | 0.657-5.878 | 0.227 |
| Age, years | 1.021 | 0.977-1.066 | 0.350 |
| DM | 0.955 | 0.402-2.274 | 0.918 |
| HTN | 0.378 | 0.130-1.095 | 0.073 |
| AKI | 1.751 | 0.749-4.092 | 0.196 |
| Baseline Cr (mg/dL) | 2.057 | 0.893-4.738 | 0.090 |
| Stone composition (based on calcium containing stone) | - | - | 0.309 |
| Urate stone | 1.640 | 0.536-5.017 | 0.386 |
| Struvite stone | 2.632 | 0.762-9.088 | 0.126 |
| Note: CI: Confidence Interval; DM: Diabetes Mellitus; HTN: Hypertension; AKI: Acute Kidney Injury; Cr: Creatinine. Multivariate cox regression was performed to adjust for sex, age, diabetes mellitus, hypertension, baseline serum creatinine, stone composition, and acute kidney injury. | |||
Table 7: Cox regression analysis of factors associated with mortality.
| For kidney function deterioration | Hazard ratio | 95% CI | p-value |
|---|---|---|---|
| Sex (Female to male) | 1.992 | 1.032-3.845 | 0.040 |
| Age, years | 1.047 | 1.016-1.078 | 0.002 |
| DM | 0.832 | 0.423-1.634 | 0.593 |
| HTN | 0.880 | 0.398-1.944 | 0.752 |
| AKI | 7.887 | 2.719-22.880 | <0.001 |
| Baseline Cr (mg/dL) | 2.103 | 1.477-2.995 | <0.001 |
| Stone composition (based on calcium containing stone) | - | - | 0.263 |
| Urate stone | 0.720 | 0.333-1.556 | 0.403 |
| Struvite stone | 0.454 | 0.169-1.222 | 0.118 |
| Note: CI: Confidence Interval; DM: Diabetes Mellitus; HTN: Hypertension; AKI: Acute Kidney Injury; Cr: Creatinine. Multivariate cox regression was performed to adjust for sex, age, diabetes mellitus, hypertension, baseline serum creatinine, stone composition, and acute kidney injury. | |||
Table 8: Cox regression analysis of factors associated with kidney function deterioration.
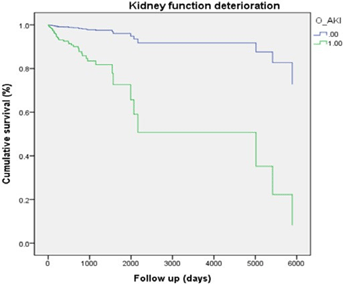
Figure 1: Kaplan-Meier survival curve comparing the AKI and non-AKI groups. Cumulative probability of kidney function deteriora tion, indicating a significant difference between the groups (HR=7.887, 95% CI 2.719-22.880, p<0.001).
DISCUSSION
Urinary stone disease is increasingly recognized as a chronic medical condition associated with AKI, CKD, ESKD, and other metabolic diseases. Previous studies were largely population based historical cohort studies that used diagnostic codes without considering stone types, clinical symptoms, or concurrent AKI. Our study included 725 symptomatic patients who underwent stone removal procedures and had known stone composition. Our key findings were as follows: 1) AKI was frequently complicated in symptomatic stone disease (35.3%); 2) higher baseline serum creatinine levels, lower albumin and hemoglobin levels, and urate struvite stone compositions were independent risk factors of AKI; and 3) during the mean follow-up of 852.2 days, 5.8% of patients showed more than a 30% decrease in eGFR, with older age, female gender, high baseline serum creatinine levels, and concurrent AKI episodes identified as risk factors. Conversely, the stone subtypes were not independent predictors of kidney function deterioration.
Urinary stones are formed through mechanisms involving crystal nucleation, supersaturation, crystal growth, and agglomeration [16]. The location and composition of nucleation are heterogeneous and can influence the clinical manifestations of urinary stone disease. Although obstruction might be one of the single most important factors causing AKI, the etiologies of AKI in patients with urinary stone disease are often multifactorial, including a combination of urinary tract infection, volume depletion, and use of nephrotoxic agents such as non-steroidal anti-inflammatory drugs (NSAIDs) and contrasts [17,18]. However, due to the retrospective nature of our study, detailed etiological classifications of AKI were not feasible. Thus, our results should be interpreted with caution. We found a significantly higher incidence of AKI in the urate and struvite stone subgroups. The percentage of stage 3 AKI was also the highest in patients with urate stones, followed by those with struvite stones while patients with calcium containing stones had the lowest percentage of stage 3 AKI out of the three stone subgroups. Older age, higher CKD prevalence, and comorbidities in patients with urate stones, may have contributed to a higher incidence of AKI in the urate stone subgroup. Similarly, concurrent infections in patients with struvite stones may have contributed to a higher AKI incidence. However, the associations between the stone compositions and the AKI incidence remained independent after adjusting for multiple factors. The lack of information regarding the location or bilaterality of stones, which can also affect AKI, is one of the limitations of our study. In addition to stone subtypes, we also found that higher baseline serum creatinine and uric acid levels, as well as lower albumin and hemoglobin levels, were independently associated with AKI in patients with urinary stone disease.
Most population-based studies have consistently shown a higher risk of CKD in patients with urinary stone disease [19]. We also observed that 5.8% of patients showed a more than 30% decrease in eGFR during the mean follow-up of 852.2 days. Using the data from the National Health Insurance Service (NHIS) of Korea, including 219,570 Korean adults with urinary stone disease and age- and sex-matched controls, Kim et al. recently demonstrated that patients with urinary stone disease have a higher risk of incident CKD than those without stones [20]. Although further studies are needed, they speculate that the progressive scarring of the kidneys from the obstructive uropathy, inflammation caused by the crystal deposition and underlying metabolic disorders prone to CKD may all contribute to the development and progression of CKD in patients with urinary stone disease. Based on the different baseline clinical and laboratory characteristics and incidence rates of AKI, we hypothesized that the rate of kidney function deterioration may also differ according to stone subtypes. However, our results demonstrated that stone subtypes were not independently associated with the rate of kidney function deterioration. Based on the current analysis, it is not possible to determine whether stone composition is a causal factor of kidney function deterioration or a marker reflecting underlying comorbidities. This represents a limitation of our study and highlights the need for further evaluation to establish a clear causal relationship.
Instead, we found that the female gender, older age, AKI, and higher baseline serum creatinine levels was an independent predictor of kidney function deterioration. Recent studies have reported that female stone formers may be more susceptible to renal impairment, potentially due to a post-menopausal loss of estrogen-mediated renoprotection and sex-specific differences in infection risk and health care utilization [21]. Higher CKD susceptibility in female stone formers was also demonstrated in a population-based study performed in England and Wales and a meta-analysis [22,23]. Interestingly, these findings are contrary to a recently published study that included data from the National Health Insurance Service of Korea database which reported that men had a greater risk of developing CKD when compared to women [24]. Similarly, Ricardo et al. also suggested that men were more susceptible to CKD progression [25]. Further studies are necessary to clarify gender differences and CKD susceptibility in patients with stones.
In contrast to CKD, the association between urinary stone disease and mortality remains unclear. A large population-based study from the United States using data from the National Health and Nutrition Examination Survey [26] demonstrated more than a two-fold increase in the risk of all-cause and cardiovascular mortality in their unadjusted analysis. However, the association was no longer present after adjusting for multiple socioeconomic and comorbid conditions, suggesting that the increased risk of mortality in patients with urinary stones may be attributed to their underlying comorbidities. In our study, we found that all-cause mortality was the highest among patients with urate stones, followed by those with struvite stones, with those with calcium stones having the lowest all-cause mortality. However, after adjusting for other comorbidities, stone subtypes were not independently associated with mortality. These findings may be partly associated with the relatively small number of patients in our study. Further studies with larger number of patients are warranted.
Our study has several strengths. First, we included hospitalized patients with symptomatic kidney stone disease who underwent stone removal procedures which allowed us to perform analyses according to different stone compositions. This approach enabled us to obtain comprehensive demographic and laboratory data both before and after the occurrence of the stone, allowing for the assessment of the impact of the stone composition on various outcomes. Second, we assessed AKI occurring at the time of stone removal and found that a concurrent AKI episode is independently associated with long-term kidney function deterioration. These findings support the concept that kidney stone disease should not be regarded as a one-time condition, but rather as a chronic disease that requires long-term renal function monitoring, imaging follow-up, and appropriate comorbidity management to prevent recurrence, particularly in patients who have experienced urinary stone combined with AKI.
This study also has several limitations. First, as a single-center retrospective study, generalizability of our findings may be limited. Second, kidney function deterioration was defined based on the difference between the baseline eGFR and the eGFR calculated from the last serum creatinine measurement during the study period. Therefore, the outcome may not fully reflect the true CKD progression, as recurrent AKI or early loss to follow up at the time of the last measurement may have confounded our results. Third, information regarding stone location, bilaterality, stone size, type of intervention, and recurrence was not included in the analysis, which may have limited the comprehensive assessment of disease progression and risk stratification.
CONCLUSION
This study showed different clinical outcomes according to stone compositions. Urate and struvite stone are independent risk factor of concurrent AKI. And this AKI episode, older age, and lower baseline kidney function were independent predictors of progressive kidney function deterioration, regardless of stone composition. These results establish a foundation for future studies and may ultimately guide personalized risk stratification and preventive strategies to mitigate both acute and chronic kidney outcomes in stone formers. Future studies with longer follow-up periods and larger, more diverse study populations will be essential to refine the understanding of kidney function deterioration and to clarify risk factors affecting short and long term kidney outcomes.
ACKNOWLEDGEMENTS
This study was supported by the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education (RS-2022-NR070214). Baseline data of patients were provided by the Medical Information Team of Korea University Anam Hospital. Additional data regarding ESKD progression were collected from the registry of the Korean Society of Nephrology, and the National Database of Statistics, Korea. The authors thank all investigators and coordinators in Korea University Anam Hospital. Also, we would like to thank Editage (www.editage.co.kr) for English language editing.
AUTHOR CONTRIBUTIONS
Conceptualization, Investigation: YEC, JY, S-KJ
Data acquisition: YEC, JY, YJ, M-GK
Formal data analysis, interpretation: YEC, SWO, TYK, S-KJ
Supervision: S-KJ
Writing-original draft: YEC, S-KJ
Writing-review & editing: YEC, JY, YJ, TYK, SWO, M-GK, S-KJ
All authors read and approved the final manuscript.
FUNDING SOURCE
This study was supported by the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education (RS-2022-NR070214).
DATA AVAILABILITY
The data presented in this study are available from the authors upon reasonable request.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study protocol was approved by the Institutional Review Board (IRB) of Korea University Anam Hospital, Seoul, Republic of Korea (2022AN0310), and was conducted in accordance with the principles of the Declaration of Helsinki. Informed consent was waived due to the retrospective nature of the study.
COMPETING INTERESTS
The authors have no conflicts of interest to declare.
REFRENCES
- Scales Jr CD, Smith AC, Hanley JM, Saigal CS, Urologic Diseases in America Project. Prevalence of kidney stones in the United States. Eur Urol. 2012;62(1):160-165.
- Croppi E, Ferraro PM, Taddei L, Gambaro G, GEA Firenze Study Group. Prevalence of renal stones in an Italian urban population: A general practice-based study. Urol Res. 2012;40(5):517-522.
[Google Scholar] [PubMed] [Crossref]
- Zeng G, Mai Z, Xia S, Wang Z, Zhang K, Wang L, et al. Prevalence of kidney stones in China: An ultrasonography based cross‐sectional study. BJU Int. 2017;120(1):109-116.
[Google Scholar] [PubMed] [Crossref]
- Tae BS, Balpukov U, Cho SY, Jeong CW. Eleven-year cumulative incidence and estimated lifetime prevalence of urolithiasis in Korea: A National Health Insurance Service-national sample cohort based study. J Korean Med Sci. 2018;33(2):e13.
[Google Scholar] [PubMed] [Crossref]
- Tang X, Lieske JC. Acute and chronic kidney injury in nephrolithiasis. Curr Opin Nephrol Hyperten. 2014;23(4):385-390.
[Google Scholar] [PubMed] [Crossref]
- El-Zoghby ZM, Lieske JC, Foley RN, Bergstralh EJ, Li X, Melton III LJ, et al. Urolithiasis and the risk of ESRD. Clin J Am Soc Nephrol. 2012;7(9):1409-1415.
[Google Scholar] [PubMed] [Crossref]
- Yang J, Sun BG, Min HJ, Son YB, Kim TB, Lee J, et al. Impact of acute kidney injury on long-term adverse outcomes in obstructive uropathy. Sci Rep. 2021;11(1):23639.
[Google Scholar] [PubMed] [Crossref]
- Shang W, Li Y, Ren Y, Yang Y, Li H, Dong J. Nephrolithiasis and risk of hypertension: A meta-analysis of observational studies. BMC nephrology. 2017;18(1):344.
[Google Scholar] [PubMed] [Crossref]
- Taylor EN, Stampfer MJ, Curhan GC. Diabetes mellitus and the risk of nephrolithiasis. Kidney Int. 2005;68(3):1230-1235.
[Google Scholar] [PubMed] [Crossref]
- Alexander RT, Hemmelgarn BR, Wiebe N, Bello A, Samuel S, Klarenbach SW, et al. Kidney stones and cardiovascular events: A cohort study. Clin J Am Soc Nephrol. 2014;9(3):506-512.
[Google Scholar] [PubMed] [Crossref]
- Oztoprak BG, Gonzalez J, Yoo J, Gulecen T, Mutlu N, Russo RE, et al. Analysis and classification of heterogeneous kidney stones using Laser-Induced Breakdown Spectroscopy (LIBS). Appl Spectrosc. 2012;66(11):1353-1361.
[Google Scholar] [PubMed] [Crossref]
- Wiederkehr MR, Moe OW. Uric acid nephrolithiasis: A systemic metabolic disorder. Clin Rev Bone Miner Metab. 2011;9(3):207-217.
[Google Scholar] [PubMed] [Crossref]
- Lieske JC, Rule AD, Krambeck AE, Williams JC, Bergstralh EJ, Mehta RA, et al. Stone composition as a function of age and sex. Clin J Am Soc Nephrol. 2014;9(12):2141-2146.
[Google Scholar] [PubMed] [Crossref]
- Levey AS, Inker LA, Matsushita K, Greene T, Willis K, Lewis E, et al. GFR decline as an end point for clinical trials in CKD: A scientific workshop sponsored by the National Kidney Foundation and the US Food and Drug Administration. Am J Kidney Dis. 2014;64(6):821-835.
[Google Scholar] [PubMed] [Crossref]
- Sontrop JM, Weir MA, Garg AX. Surrogate outcomes for ESRD risk: The case for a 30% reduction in estimated GFR over 2 years. Am J Kidney Dis. 2014;64(6):845-847.
[Google Scholar] [PubMed] [Crossref]
- Khan SR, Pearle MS, Robertson WG, Gambaro G, Canales BK, Doizi S, et al. Kidney stones. Nat Rev Dis Primers. 2016;2(1):1-23.
- Chen H, He C, You Z, Zhang S, He H, Chen XN, et al. Association between urine pH and risk of contrast-associated acute kidney injury among patients after emergency percutaneous coronary intervention: A V-shape relationship?. Clin Exp Nephrol. 2021;25(5):554-561.
[Google Scholar] [PubMed] [Crossref]
- Yoshida S, Miyake T, Yamamoto S, Furukawa S, Niiya T, Senba H, et al. Relationship between urine pH and abnormal glucose tolerance in a community‐based study. J Diabetes Investig. 2018;9(4):769-775.
[Google Scholar] [PubMed] [Crossref]
- Gambaro G, Croppi E, Bushinsky D, Jaeger P, Cupisti A, Ticinesi A, et al. The risk of chronic kidney disease associated with urolithiasis and its urological treatments: A review. J Urol. 2017;198(2):268-273.
[Google Scholar] [PubMed] [Crossref]
- Kim JY, Lee JK, Park JT, Chang TI. Risk of incident chronic kidney disease among patients with urolithiasis: A nationwide longitudinal cohort study. Clin Kidney J. 2024;17(3):sfae030.
[Google Scholar] [PubMed] [Crossref]
- Chien TM, Lu YM, Li CC, Wu WJ, Chang HW, Chou YH. A retrospective study on sex difference in patients with urolithiasis: Who is more vulnerable to chronic kidney disease?. Biol Sex Differ. 2021;12(1):40.
[Google Scholar] [PubMed] [Crossref]
- Stewart S, Kalra PA, Blakeman T, Kontopantelis E, Cranmer-Gordon H, Sinha S. Chronic kidney disease: Detect, diagnose, disclose—a UK primary care perspective of barriers and enablers to effective kidney care. BMC Med. 2024;22(1):331.
[Google Scholar] [PubMed] [Crossref]
- Lewandowski MJ, Krenn S, Kurnikowski A, Bretschneider P, Sattler M, Schwaiger E, et al. Chronic kidney disease is more prevalent among women but more men than women are under nephrological care: Analysis from six outpatient clinics in Austria 2019. Wien Klin Wochenschr. 2023;135(3):89-96.
[Google Scholar] [PubMed] [Crossref]
- Ko HJ, Ahn SK, Han S, Kim MJ, Na KR, Park H, et al. The factors influencing chronic kidney disease incidence: Database from the Korean National Health Insurance Sharing Service (NHISS). J Clin Med. 2024;13(8):2164.
[Google Scholar] [PubMed] [Crossref]
- Ricardo AC, Yang W, Sha D, Appel LJ, Chen J, Krousel-Wood M, et al. Sex-related disparities in CKD progression. J Am Soc Nephrol. 2019;30(1):137-146.
[Google Scholar] [PubMed] [Crossref]
- Tang J, Mettler P, McFann K, Chonchol M. The association of prevalent kidney stone disease with mortality in US adults: The National Health and Nutrition Examination Survey III, 1988-1994. Am J Nephrol. 2013;37(5):501-506.
[Google Scholar] [PubMed] [Crossref]
Author(s) Info
1 Department of Internal Medicine, Korea University Anam Hospital, Seoul, Korea (South)2 Department of Internal Medicine, Kangbuk Samsung Medical Center, Seoul, Korea (South)
Received date: 20-Nov-2025, Manuscript No: JNP-25-165656; Editor Assigned: 24-Nov-2025 Reviewed: 08-Dec-2025 Published date: 25-Dec-2025
Citation: Choi YE, Yang J, Jang Y, Koo TY, Oh SW, Kim MG, et al. (2025) Clinical Features and Outcomes of Symptomatic Urinary Stone Disease: An Analysis According to Stone Compositions. J Nephrol.1:13.
Copyright: © 2025 Choi YE, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
