Risk of Fatigue and Nausea in Patients with Breast Cancer Treated with Phosphatidylinositol 3-Kinase Inhibitors: A Meta-Analysis Based on Randomized Controlled Trials
Abstract
Introduction: Phosphatidylinositol 3-Kinase (PI3K) inhibitors are emerging as promising therapeutic agents for the treatment of breast cancer. Fatigue and nausea are prevalent adverse effects associated with cancer therapy. Therefore, we performed a meta analysis to elucidate the Relative Risks (RRs) of fatigue and nausea attributable to PI3K inhibitors.
Methods: Databases were searched for articles published until December 2024 reporting on phase II/III randomized controlled trials. Summary proportions and RRs for all-grade and grade 3/4 events were computed using either random-or common-effects models.
Results: We included 11 trials. There were 2427 patients with BC who received PI3K inhibitors, and 2061 received placebos. The RR for all-grades and grade 3/4 fatigue was 1.25 and 2.38, respectively. The RR of all-grade nausea was 1.73 (95% Confidence Interval [CI]). In subgroup analyses, Alpelisib significantly increased the risk of grade 3/4 nausea, and the risk of fatigue and nausea was lower in patients with Human Epidermal Growth Factor Receptor 2 (HER2) (+) BC than in those with HER2 (-) BC. The FDA Adverse Event Reporting System (FAERS) database showed that the Reporting Odds Ratios (RORs) for fatigue and nausea were 2.281 and 2.003, respectively.
Conclusion: Treatment with PI3K inhibitors increased the risk of fatigue and nausea. Given their significant impact on quality of life, early identification and appropriate management are crucial for optimizing overall treatment outcomes.
PI3K inhibitors; Alpelisib; Buparlisib; Breast cancer; Fatigue; Nausea; Adverse events
INTRODUCTION
Breast Cancer (BC) is the most common malignant tumor in women worldwide, with an increasing incidence since 2012, and has become the fourth leading cause of cancer-related deaths [1,2]. Recently, various novel agents for BC treatment, including phosphatidylinositol 3-kinase (PI3K) inhibitors, Mammalian Target of Rapamycin (mTOR) inhibitors, Cyclin-Dependent Kinase 4/6 (CDK 4/6) inhibitors, and immune checkpoint inhibitors, have been increasingly used in clinical practice. PI3K inhibitors have brought significant clinical benefits including targeting specific gene mutant tumors, overcoming resistance to CDK inhibitors and endocrine therapy, and prolonging survival time in BC treatment [3,4].
Based on structural characteristics and substrate specificity, mammals express three classes of PI3K enzymes: class IA, which includes three catalytic subunits (p110α, β, δ); class IB, which includes the P110γ subunit; class II, which includes three isoforms (PI3K-C2α, β, γ); and a single class III (hVPS34).
Class I PI3K is maintained in an inactive state by the binding of regulatory subunits to catalytic subunits. Class IA is activated by the recognition and binding of Receptor Tyrosine Kinases (RTKs), cytokine receptors, and adaptor proteins, whereas G protein-coupled receptors activate subclass 1B. Using ATP, the activated p110 subunit catalyzes the conversion of phosphatidylinositol 4,5-bisphosphate (PIP2) to the second messenger phosphatidylinositol (3,4,5)-trisphosphate (PIP3), which recruits downstream effector proteins, including Protein Kinase B (AKT, PKB). Phosphatase and tensin homolog (PTEN) mediates the dephosphorylation of PIP3. Subsequently, AKT is phosphorylated by phosphoinositide-dependent protein kinase 1 (PDK1) or the mTOR complex 2 (mTORC2), which further activates downstream mTOR via inhibition of the Tuberous Sclerosis Complex 1/2 (TSC1/2) complex. Diverse transcription factors are upregulated, leading to protein synthesis, cell growth, and motility. In humans, aberrant activation of the PI3K signaling pathway often leads to cancer, driven by mechanisms such as activating mutations in PIK3CA (a gene encoding the p110α catalytic subunit), loss-of-function mutations in PTEN (the second most frequently mutated tumor suppressor gene), and amplification and activation of human epidermal growth factor receptor 2 (HER2) [5–7].
Based on their pharmacological mechanisms, inhibitors targeting PI3K can be categorized into four major classes: (1) Pan-PI3K inhibitors, which inhibit all four isoforms of class I PI3Ks. Examples include buparlisib (BKM-120) and pictilisib (GDC 0941) [8,9]. (2) Dual PI3K inhibitors and isoform-sparing PI3K inhibitors preferentially inhibit two or three PI3K isoforms, such as taselisib (GDC-0032) [10]. (3) Isoform-selective PI3K inhibitors, such as Alpelisib (BYL719) and Inavolisib (GDC 0077), specifically target the α subunit [11]. (4) Multitarget inhibitors (excluded from this analysis), which inhibit PI3K isoforms and target other proteins, such as PI3K/mTOR inhibitors and PI3K/DNA-dependent protein kinase inhibitors.
However, these drugs can cause multiple systemic adverse events (AEs). Hyperglycemia, rash, diarrhea, fatigue, and nausea are the most common AEs associated with PI3K inhibitors in patients with BC [12]. Hyperglycemia, rash, and diarrhea are objective symptoms that may cause organic damage, requiring immediate medical attention and effective control through targeted treatments. In contrast, fatigue and nausea are more subjective, lack standardized pharmacological interventions, and are relatively mild, rarely causing organic damage; this can lead to resulting clinical neglect, allowing them to persist or progress. Fatigue is a state of generalized weakness with a pronounced inability to summon sufficient energy to accomplish daily activities, as defined by the Common Terminology Criteria for Adverse Events (CTCAE) v5.0. It is related to medication and treatment schedules and may be exacerbated by other AEs (e.g., pain, depression/anxiety, or gastrointestinal toxicity). It affects maximal oxygen uptake, cytokine, and cortisol levels, damaging mood, cognition, and social interactions, ultimately significantly reduces patients’ Quality of Life (QOL) during and after treatment and overall therapeutic efficacy [13–16]. Nausea is a queasy sensation and/or the urge to vomit associated with tumor location, therapeutic agents, a previous history of chemotherapy-induced nausea, age, and sex. It can result in nutritional and metabolic disorders, anorexia, deterioration of physical and mental conditions, dose reduction or discontinuation of chemotherapy, abandonment of potentially beneficial cancer treatments, and increased anxiety and diminished QOL, ultimately complicating treatment [17-18]. The outcomes of nausea are inextricably linked to the occurrence of fatigue and both significantly impair patients’ QOL. In the European Organization for Research and Treatment of Cancer QLQ-C30, fatigue, nausea, and vomiting are listed as symptom subscales to more accurately reflect patients’ actual experiences and needs [19].
Thus, we aimed to investigate the risk of fatigue and nausea associated with PI3K inhibitors in the treatment of BC through an updated meta-analysis and systematic review of Randomized Controlled Trials (RCTs). We compiled and analyzed existing clinical trial data for different drugs, AE grades, and other aspects.
METHODS
Data source
A systematic literature search was independently performed by two investigators using electronic databases including PubMed/ Medline, Web of Science, Embase, and the Cochrane Controlled Trials Register (CENTRAL) from their inception to December 2024. The search strategy was: ((breast cancer) OR (breast tumor) OR (breast tumors) OR (breast neoplasm) OR (breast neoplasms) OR (breast carcinomas) OR (breast carcinoma) OR (CARCINOMA OF BREAST) OR (Mammary Carcinoma) OR (Mammary Neoplasms)) AND (PI3K OR PI3-Kinase OR (Phosphatidylinositol 3-kinase) OR (phosphatidylinositol 3-kinase) OR (phosphatidylinositol 3-kinases) OR PI3KBeta OR p110-ALPHA) AND (inhibitor OR inhibitors) AND ((adverse reactions) OR (adverse events) OR (adverse effects) OR (adverse occurrences) OR (adverse incidents) OR (drug-related side effects) OR (adverse drug reaction) OR (adverse drug reactions)). We searched abstracts and virtual meeting presentations from the American Society of Clinical Oncology and the European Society of Medical Oncology held from the databases’ inception to December 2024. Furthermore, we searched the clinical trial registration website (http://www.ClinicalTrials.gov) to obtain information on prospectively registered trials, checked the reference lists of topic-related reviews, and identified eligible studies. When multiple publications from the same clinical trial were identified, we used the most recent or complete report. The literature search was updated immediately before the final analysis.
Inclusion and exclusion criteria
Studies meeting the following eligibility criteria were included: (1) articles published in English, (2) prospective phase II or III RCT involving patients with BC, (3) participants assigned to treatment with PI3K inhibitors (excluding multitarget inhibitors) or placebos, (4) and studies with available safety data reporting AEs. Conference abstracts were considered if they provided sufficient information on the study design, participant characteristics, interventions, outcomes, and toxicity profiles. The full texts of potentially relevant studies were retrieved, and the methods and results were reviewed for trial design and reporting of fatigue and nausea. Single-arm and randomized clinical trials with PI3K inhibitors in both arms were excluded due to the lack of appropriate control groups.
Data extraction and quality assessment
Two reviewers independently extracted the essential data in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Any discrepancies were resolved through consensus. The following variables were extracted from each eligible study: first author’s name, publication year, register ID, trial phase, classification and staging of BC, number of enrolled patients, dosage regimens used in the PI3K inhibitor and control arms, CTCAE version, blinding, withdrawals, number of patients for analysis, and incidence of selected AEs.
Data on the occurrence of AEs were obtained from the safety profiles or supplemental materials of each study. Data on all grade and grade 3/4 fatigue and nausea events were collected for each eligible study. AE grading was defined according to the National Cancer Institute’s CTCAE (version 5; http://ctep. cancer.gov). The methodological quality of the included trials was assessed using the revised Cochrane risk-of-bias version 2 tool (RoB 2.0). Studies were categorized as having “low risk,” “high risk,” or “some concerns” across the six specified domains. The risk of bias assessment is presented in (Figure 1).
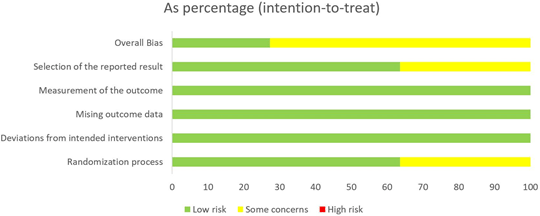
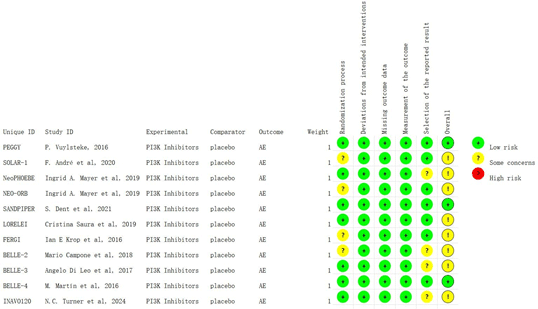
Figure 1: Risk of bias assessment of all included randomized studies.
Statistical analysis
For the calculation of Relative Risks (RRs) and 95% Confidence Intervals (CIs), the number of patients receiving PI3K inhibitors versus placebo and the number of patients with all-grade fatigue and nausea events were extracted from the selected clinical trials. The proportion of patients with each adverse outcome was calculated for each trial. Nine trials investigated doses that are not currently approved. To examine the characteristics of the specific AE grades within subgroups and to verify the consistency between subgroup results and overall sample, we conducted a subgroup analysis of these trials [8–11, 20–24].
Heterogeneity was assessed using the Q statistic and I2 metric. A P-value of less than 0.05 was considered indicative of substantial heterogeneity. I2 values of 25%, 50%, and 75% indicated low, moderate, and high heterogeneity, respectively. When substantial heterogeneity was not observed, a common-effect model was applied using the Mantel-Haenszel method. When substantial heterogeneity was observed, a random-effects model was applied using the DerSimonian and Laird method, which accounts for both within-study and between-study variance. Funnel plots were used to visually assess publication bias, and Begg’s test was used to quantify it. A two-tailed P-value of less than 0.05 was considered statistically significant. All statistical analyses were performed using the “meta” package in R software (version 4.4.0).
RESULTS
Search results
Our search strategy identified 179 publications that were potentially relevant to patients with BC treated with PI3K inhibitors. After removing duplicates, phase I/IV clinical trials, non-RCTs, and studies involving multitarget inhibitors, and screening the titles and abstracts, 146 manuscripts were excluded for not meeting the inclusion criteria, leaving 33 selected for further review. Upon subsequent screening, an additional 8 records were excluded due to being trials in progress or providing only grade 1–3 AE data. After the selection process, 11 RCTs were deemed eligible for inclusion in the meta-analysis. The selection process is illustrated in (Figure 2).
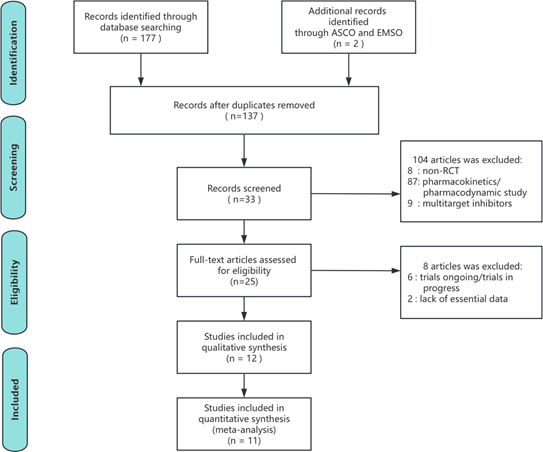
Figure 2: PRISMA flowchart illustrating the selection of studies included in the present analysis. The illustration shows the number of records obtained from the database and final number of the studies included in the analysis. Note: ASCO = American Society of Clinical Oncology; ESMO = European Society for Medical Oncology; RCT = Randomized Controlled Trial.
Study quality
The included studies were published between 2016 and 2024. All were randomized trials, comprising six phase II and f ive phase III studies, and all 11 were published as full-text manuscripts. Using the Cochrane Collaboration’s risk-of-bias tool, we assessed the quality of the included studies as good or fair, with no studies graded as having a high risk of bias across the six specified domains. All 11 trials reported AEs according to the National Cancer Institute’s CTCAE, using either version 4, version 5, or unspecified criteria (as in the FERGI, BELLE-2, and Neo PHOEBE trials).
Patients
The baseline characteristics of the included trials are summarized in (Table 1). In total, 4488 patients were included in this meta analysis (PI3K inhibitors: 2427; controls/placebo: 2061). Patients included in those trials followed the eligibility criteria defined by each unique trial, which generally included: postmenopausal status defined as prior bilateral oophorectomy; age ≥60; or age <60 with amenorrhea for ≥12 months according to National Comprehensive Cancer Network guidelines; Measurable disease or non-measurable lytic or mixed bone lesions according to Response Evaluation Criteria in Solid Tumors (RECIST, version 1.1); overall survival including confirmed objective response, best overall response, clinical benefit, and response duration according to RECIST; Progression-Free Survival (PFS) defined as the time from randomization to the first occurrence of disease progression according to RECIST; a diagnostic biopsy for PIK3CA mutation status (using the Cobas® PIK3CA Mutation Test) and Ki-67 level; Eastern Cooperative Oncology Group performance status of 0–2; adequate bone marrow, glucose metabolism, hematological, and organ function; and acceptance of endocrine therapy alone at the time of study entry, per treatment guidelines. All 11 included trials reported safety data on fatigue Table 2, and 10 trials reported safety data on nausea Table 3, which were analyzed separately. Two trials combined a PI3K inhibitor with new-generation aromatase inhibitors (letrozole or anastrozole), 1 trial combined it with the CDK4/6 inhibitor palbociclib, and 2 trials combined a PI3K inhibitor with trastuzumab and paclitaxel or with palbociclib and fulvestrant. The PI3K inhibitor doses used in the studies were 300 mg QD for alpelisib, 100 or 80 mg QD for buparlisib, 4 mg QD for taselisib, 340 or 260 mg QD for pictilisib, and 9 mg QD for inavolisib. A capsule formulation was used in 2 trials, and tablet formulations were used in 2 others.
| Author, year | Trial name | Trial number | Study design | Condition | PI3K Inhibitors |
Author, year | Dose frequency | Duration | Cycle | Control drug | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Inhibitor class | Drug dosage | ||||||||||
| Ingrid A. Mayer et al, 2019 | NEO-ORB | NCT01923168 | Phase 2 RCT | HR-positive, HER2- negative locally breast cancer |
Alpelisib + Letrozole | Isoform- selective α |
300 mg/d | Earlier stage: QD; From January 29, 2015: QD, 5 days on/ 2 days off |
24 weeks | NC | Placebo + Letrazole |
| F. André et al, 2020 | SOLAR-1 | NCT02437318 | Phase 3 RCT |
HR-positive, HER2- negative advanced breast cancer |
Alpelisib + Fulvestrant |
Isoform- selective α |
300 mg/d | QD | Treatment until disease progression, an unacceptable level of toxic effects, withdrawal of consent, loss to follow-up, or death |
1 cycle=28d (±3 days) |
Placebo + Fulvestrant |
| Sibylle Loibl et al, 2017 | Neo PHOEBE | NCT01816594 | Phase 2 RCT | HER2- positive breast cancer |
Buparlisib + Trastuzumab + Paclitaxel | Pan | The first 6 weeks: 100 mg/day; The rest 12 weeks: 80 mg/d |
QD | 18 weeks | NC | Placebo + Trastuzumab + Paclitaxel |
| M. Martín et al, 2016 |
BELLE-4 | NCT01572727 | Phase 2 RCT | HER2- negative locally advanced or metastatic breast cancer |
Buparlisib + Paclitaxel |
Pan | 100 mg/d | QD | Treatment until disease progression, unacceptable toxicity, death, or discontinuation for any other reason |
1 cycle=28d |
Placebo + Paclitaxel |
| Angelo Di Leo et al, 2017 | BELLE-3 | NCT01633060 | Phase 3 RCT |
HR-positive, HER2- negative locally advanced or metastatic breast cancer |
Buparlisib + Fulvestrant |
Pan | 100 mg/d | QD | Treatment until disease progression, unacceptable toxicity, death, or discontinuation for any other reason |
1 cycle=28d |
Placebo + Fulvestrant |
| Mario Campone et al, 2018 | BELLE-2 | NCT01610284 | Phase 3 RCT |
HR-positive, HER2- negative advanced breast cancer |
Buparlisib + Fulvestrant |
Pan | 100 mg/d | QD, starting from day 15 of cycle 1 |
Treatment until disease progression, unacceptable toxicity, death, or discontinuation for any other reason |
1 cycle=28d |
Placebo + Fulvestrant |
| Cristina Saura et al, 2019 | LORELEI | NCT02273973 | Phase 2 RCT | ER-positive, HER2- negative early-stage breast cancer |
Taselisib + Letrozole | Isoform- selective α |
4 mg/d | QD, 5 days-on, 2 days-off |
16 weeks | NC | Placebo + Letrozole |
| S. Dent et al, 2021 |
SANDPIPER | NCT02340221 | Phase 3 RCT |
ER-positive, HER2- negative locally advanced or metastatic breast cancer |
Taselisib + Fulvestrant |
Isoform- selective α |
4 mg/d | QD | Treatment until progressive disease or unacceptable toxicity | 1 cycle=28d |
Placebo + Fulvestrant |
| Ian E Krop et al, 2016 | FERGI | NCT01437566 | Phase 2 RCT | ER-positive, HER2- negative locally advanced or metastatic breast cancer |
Pictilisib + Fulvestrant |
Pan | 340 mg/d | QD, starting on day 15 of cycle 1 | Treatment until disease progression, intolerable toxicity, elective withdrawal from the study, or study completion or termination |
1 cycle=28d |
Placebo + Fulvestrant |
| P. Vuylsteke et al, 2016 |
PEGGY | NCT01740336 | Phase 2 RCT | HR-positive, HER2- negative locally metastatic breast cancer |
Pictilisib + Paclitaxel |
Pan | 260 mg/d | QD, on days 1-5 every week | Treatment until progression of disease, unacceptable toxicity, study withdrawal, or study completion or termination |
1 cycle=28d |
Placebo + Paclitaxel |
| N.C. Turner et al, 2024 |
INAVO120 | NCT04191499 | Phase 3 RCT |
HR-positive, HER2- negative locally advanced or metastatic breast cancer |
Inavolisib + Palbociclib + Fulvestrant | Isoform- selective α |
9 mg/d | QD | Treatment until disease progression, unacceptable toxic effects, withdrawal of consent, or death |
1 cycle=28d |
Placebo + Palbociclib + Fulvestrant |
Table 1: Characteristics of randomized controlled trials included in the Meta-analysis. Abbreviations: QD, once per day; NC, data not collected; PI3K, phosphoinositide 3 kinase.
| Author, year | Study design | Condition | Treatment Arms | Fatigue | ||||
|---|---|---|---|---|---|---|---|---|
| PI3K Inhibitor, n |
Control / Placbo, n | PI3K Inhibitor, n (%) | Control / Placbo, n (%) | |||||
| All grades | Grade 3/4 | All grades | Grade 3/4 | |||||
| Ingrid A. Mayer et al, 2019 | Phase 2 RCT | HR-positive, HER2- negative locally breast cancer | 130 | 125 | 53(40.8) | 2(1.5) | 42 (33.6) | 1 (0.8) |
| F. André et al, 2020 | Phase 3 RCT | HR-positive, HER2- negative advanced breast cancer | 284 | 287 | 72 (25.4) | 10 (3.5) | 51 (17.8) | 3 (1.0) |
| Sibylle Loibl et al, 2017 | Phase 2 RCT | HER2-positive breast cancer |
25 | 25 | 13 (52.0) | 0 (0.0) | 14 (56.0) | 1 (4.0) |
| M. Martín et al, 2016 | Phase 2 RCT | HER2-negative locally advanced or metastatic breast cancer | 202 | 201 | 67 (33.2) | 12 (5.9) | 64 (31.8) | 6 (3.0) |
| Angelo Di Leo et al, 2017 | Phase 3 RCT | HR-positive, HER2- negative locally advanced or metastatic breast cancer | 288 | 140 | 67(23.3) | 10(3.5) | 26(18.6) | 2 (1.4) |
| Mario Campone et al, 2018 | Phase 3 RCT | HR-positive, HER2- negative advanced breast cancer | 573 | 570 | 188 (32.8) | 30 (5.2) | 143 (25.1) | 9 (1.6) |
| Cristina Saura et al, 2019 | Phase 2 RCT | ER-positive, HER2- negative early-stage breast cancer | 167 | 167 | 33(19.8) | 0(0.0) | 40(24.0) | 0(0.0) |
| S. Dent et al, 2021 | Phase 3 RCT | ER-positive, HER2- negative locally advanced or metastatic breast cancer | 416 | 213 | 101 (24.3) | \ | 38 (17.8) | \ |
| Ian E Krop et al, 2016 | Phase 2 RCT | ER-positive, HER2- negative locally advanced or metastatic breast cancer | 89 | 79 | \ | 7 (7.9) | \ | 0(0.0) |
| P. Vuylsteke et al, 2016 | Phase 2 RCT | HR-positive, HER2- negative locally metastatic breast cancer | 91 | 92 | \ | 1(1.1) | \ | 3(3.3) |
| N.C. Turner et al, 2024 | Phase 3 RCT | HR-positive, HER2- negative locally advanced or metastatic breast cancer | 162 | 162 | 38 (23.5) | 0(0.0) | 21 (13.0) | 2 (1.2) |
Table 2: The number and proportion of treatment-related fatigue in patients treated with placebo/control and PI3K inhibitors.
| Author, year | Study design | Condition | Treatment Arms | Nausea | ||||
|---|---|---|---|---|---|---|---|---|
| PI3K Inhibitor, n |
Control / Placbo, n | PI3K Inhibitor, n (%) | Control / Placbo, n (%) | |||||
| All grades | Grade 3/4 | All grades | Grade 3/4 | |||||
| Ingrid A. Mayer et al,2019 | Phase 2 RCT | HR-positive, HER2- negative locally breast cancer | 130 | 125 | 57 (43.8) | 2 (1.5) | 23 (18.4) | 0(0.0) |
| F. André et al,2020 | Phase 3 RCT | HR-positive, HER2- negative advanced breast cancer | 284 | 287 | 133 (46.8) | 8 (2.8) | 65 (22.6) | 1 (0.3) |
| Sibylle Loibl et al,2017 | Phase 2 RCT | HER2-positive breast cancer |
25 | 25 | 11 (44.0) | 0 (0.0) | 8 (32.0) | 0 (0.0) |
| M. Martín et al,2016 |
Phase 2 RCT | HER2-negative locally advanced or metastatic breast cancer | 202 | 201 | 83 (41.1) | 1 (0.5) | 51 (25.4) | 2 (1.0) |
| Angelo Di Leo et al,2017 | Phase 3 RCT | HR-positive, HER2- negative locally advanced or metastatic breast cancer | 288 | 140 | 99 (34.4) | 3 (1.0) | 25 (17.9) | 3 (2.1) |
| Mario Campone et al,2018 | Phase 3 RCT | HR-positive, HER2- negative advanced breast cancer | 573 | 570 | 228 (39.8) | 11 (1.9) | 138 (24.2) | 8 (1.4) |
| Cristina Saura et al,2019 | Phase 2 RCT | ER-positive, HER2- negative early-stage breast cancer | 167 | 167 | 35 (21.0) | 1 (0.6) | 19 (11.4) | 0(0.0) |
| S. Dent et al,2021 |
Phase 3 RCT | ER-positive, HER2- negative locally advanced or metastatic breast cancer | 416 | 213 | 142 (34.1) | \ | 52 (24.4) | \ |
| Ian E Krop et al,2016 | Phase 2 RCT | ER-positive, HER2- negative locally advanced or metastatic breast cancer | 89 | 79 | \ | 3 (3.4) | \ | 0(0.0) |
| N.C. Turner et al,2024 | Phase 3 RCT | HR-positive, HER2- negative locally advanced or metastatic breast cancer | 162 | 162 | 45 (27.8) | 1 (0.6) | 27 (16.7) | 0(0.0) |
Table 3: The number and proportion of treatment-related nausea in patients treated with placebo/control and PI3K inhibitors.
Relative risk of fatigue
A common-effect model was applied. Treatment with PI3K inhibitors significantly increased the risk of all-grade fatigue (RR = 1.25, 95% CI: 1.12–1.38; I2 = 21.7%) and grade 3/4 fatigue (RR = 2.38, 95% CI: 1.54–3.66; I2 = 16.7%) (RR>1 indicates an increased risk) compared to placebo/control, respectively (Figure 3A, 3C). Funnel plots were symmetric for both outcomes, and P-values from Begg’s test were 0.75 for all grade and 0.35 for grade 3/4 fatigue (P>0.05; (Figure 3B, 3D), indicating no evidence of publication bias. The imputation of potentially “missing studies” did not alter the results.
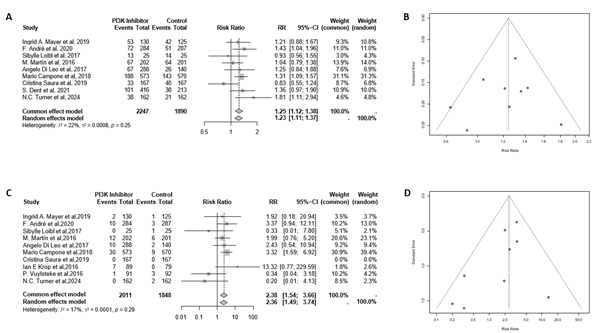
Figure 3: Forest plots and funnel plots of all-grade (A,B) and grade 3/4 (C,D) fatigue events associated with PI3K inhibitor versus placebo/control.
Subgroup analysis by specific drugs revealed a statistically significant increase in the risk of all-grade fatigue with alpelisib, buparlisib, and inavolisib separately. In contrast, the risk of grade 3/4 fatigue was not significantly increased for these three drugs compared to the placebo/control (Figure 4A, 4C). For buparlisib, the effect sizes for all-grade and grade 3/4 fatigue were similar in the original studies; the pooled analysis showed significant differences for both, with comparable effect magnitudes. Subgroup analysis by trial phase (II/III) showed that the risk of both all-grade and grade 3/4 fatigue were statistically significant in phase III trials, but not in phase II trials compared to the placebo/control (Figure 4B, 4D). In addition, for phase II clinical trials, the effects on all-grade and grade 3/4 fatigue were consistent with those reported in the original studies. Subgroup analysis by different cancer types showed that the risk of all-grade and grade 3/4 fatigue was statistically significant in patients with HER2(−) BC, but not in those with HER2(+) BC compared to placebo/control (Figure 4E, 4G). Subgroup analysis by cancer stage showed that the risk of all-grade fatigue was not significantly different in patients with early-stage BC (Figure 4F, 4H).
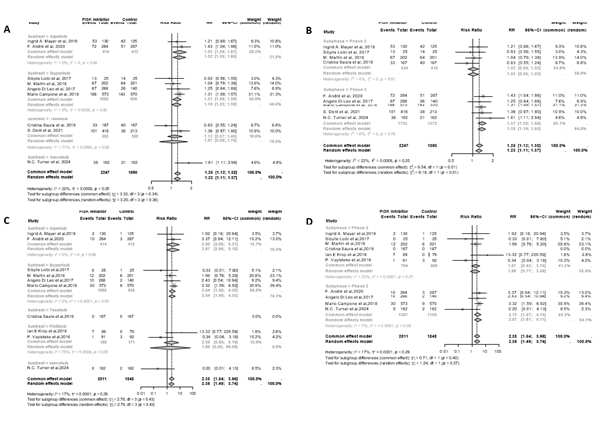
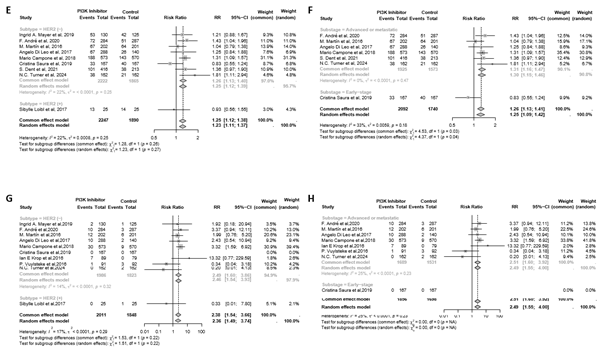
Figure 4: Forest plots of all-grade (A-B, E-F) and grade 3/4 (C-D, G-H) fatigue events associated with drugs/ phases of trials/ cancer types/ cancer stages versus placebo/control in sub-group analysis.
Relative risk of nausea
A common-effect model was applied. Treatment with PI3K inhibitors significantly increased the risk of all-grade nausea (RR = 1.73, 95% CI: 1.57–1.92; I2 = 0.0%); however, the increase in grade 3/4 nausea was not statistically significant (RR = 1.80, 95% CI: 1.00–3.22; I2 = 2.1%) (RR>1 indicates an increased risk) compared to placebo/control, respectively (Figure 5A, 5C). Funnel plots were symmetric for both outcomes, and P-values from Begg’s test were 0.92 for all-grade and 0.90 for grade 3/4 nausea (P>0.05; (Figure 5B, 5D), indicating no evidence of publication bias. The imputation of potentially “missing studies” did not alter the results.
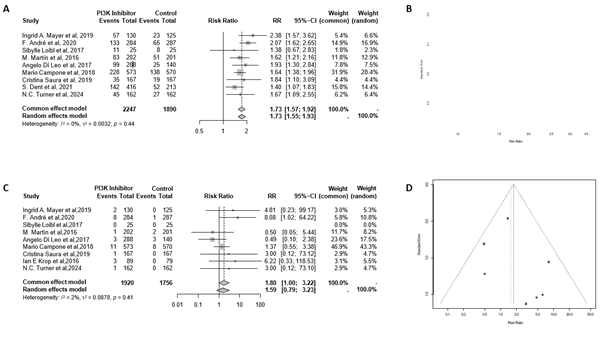
Figure 5: Forest plots and funnel plots of all-grade (A,B) and grade 3/4 (C,D) nausea events associated with PI3K inhibitor versus placebo/control.
Subgroup analysis by specific drug showed a statistically significant increase in the risk of grade 3/4 nausea with alpelisib (RR = 6.97, 95% CI: 1.27–38.31; I2 = 0.0%). The other PI3K inhibitors in the subgroup showed trends consistent with the overall sample compared to placebo/control, respectively (Figure 6A, 6C). Subgroup analyses by trial phases (II/III) and cancer stage showed trends consistent with the overall sample compared to placebo/control (Figure 6B, 6D, 6F, and 6H). Subgroup analysis by cancer type showed that the risk of all grade nausea did not significantly differ in patients with HER2(+) BC (Figure 6E, 6G).
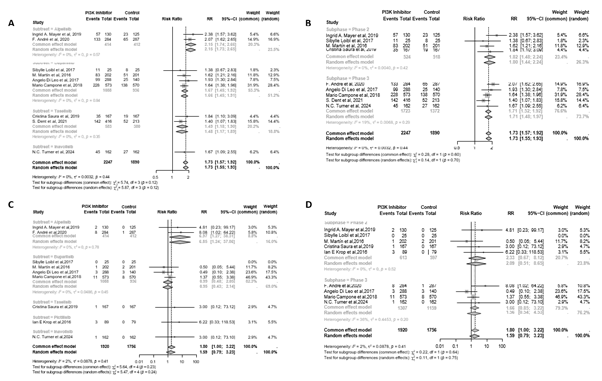
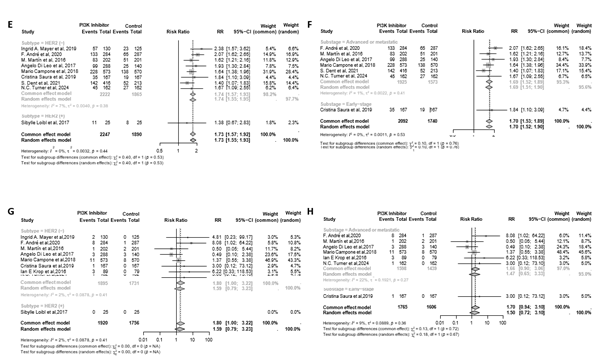
Figure 6: Forest plots of all-grade (A-B, E-F) and grade 3/4 (C-D, G-H) nausea events associated with drugs/ phases of trials/ cancer types/ cancer stages versus placebo/control in sub-group analysis.
Sensitivity analyses
Sensitivity analyses yield results consistent with the major outcomes of interest (all-grade fatigue, grade 3/4 fatigue, all grade nausea, and grade 3/4 nausea) compared to the main analyses (Figure 7, 8). As in the main analysis, the pooled effect on grade 3/4 nausea was not significant in the sensitivity analysis (Figure 8B).
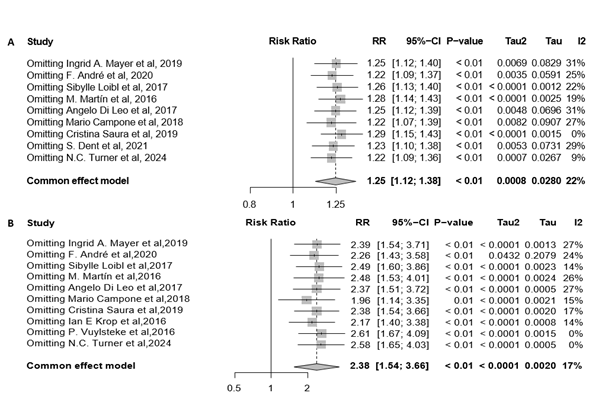
Figure 7: Forest plots of all-grade (A) and grade 3/4 (B) fatigue events in sensitivity analysis.
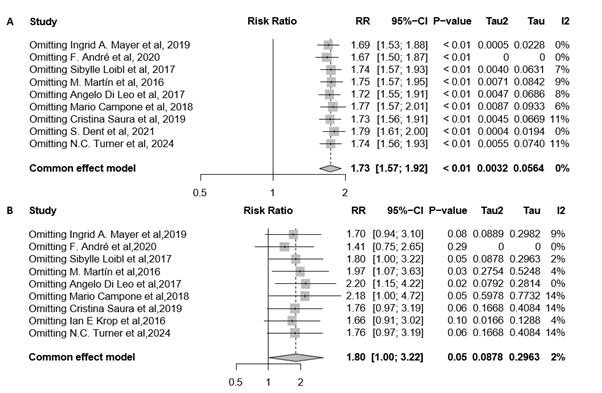
Figure 8: Forest plots of all-grade (A) and grade 3/4 (B) nausea events in sensitivity analysis.
Evidence from the FDA Adverse Event Reporting System (FAERS) database
Basic information
From the database's inception to December 31, 2024, the FARES database identified only alpelisib as a PI3K inhibitor, with data available for the treatment of BC (excluding multitarget inhibitors). A total of 803 AEs were reported for alpelisib, amounting to 6448 cases affecting 1441 individuals. Among patients with BC, fatigue was reported in 190 (13.19%) patients and nausea in 167 (11.59%) patients.
Among the 190 patients reporting alpelisib-related fatigue, the majority were female (182 [95.79%]), the most prevalent age group was 50–70 years (33 [17.37%]), and the reports were primarily from in 2021–2023 (166 [87.37%]). The primary reporting countries were the United States (125 [65.79%]), Europe (11 [5.79%]), and Asia (6 [3.16%]). Other reporting countries included Brazil (4 patients) and Egypt (1), and Canada (1). Serious AEs resulting from alpelisib treatment in patients with BC included outcomes such as death, life-threatening disease, disability, and initial or prolonged hospitalization. Among patients experiencing fatigue, 34 (17.89%) individuals had serious AE effects during hospitalization. Among the 167 patients reporting alpelisib-related nausea caused by alpelisib, females constituted the vast majority (161 [96.41%]), the most prevalent age group was 50–70 years (33 [19.76%]), with reports predominantly from 2021–2023 (157 [94.01%]). The primary countries reporting alpelisib-related AEs for nausea were the US (110 [65.87%]), Europe (11 [6.59%]), and Asia (5 [2.99%]). The other reporting countries included Brazil with 5 patients. Among patients experiencing nausea, 23 (13.77%) individuals had serious AE outcomes of hospitalization, and 3 (1.80%) individuals experienced death. The characteristics of participants experiencing fatigue and nausea are detailed in (Table 4).
| Clinical characteristics | Total [(N =190) %] |
|---|---|
| Gender | |
| Male | 3(1.58%) |
| Female | 182(95.79%) |
| Unknown | 5(2.63%) |
| Age, years | |
| ≥18Y & <50Y | 3(1.58%) |
| ≥50Y & <70Y | 33(17.37%) |
| ≥70Y | 24(12.63%) |
| Unknown | 130(68.42%) |
| Outcome | |
| Death | 1(0.53%) |
| Hospitalization | 34(17.89%) |
| Life-Threatening | 1(0.53%) |
| Other Outcomes | 154(81.05%) |
| Area & Country | |
| Africa | |
| Egypt | 1(0.53%) |
| Asia | |
| Israel | 3(1.58%) |
| Taiwan | 1(0.53%) |
| Others | 2(1.05%) |
| Europe | |
| Russia | 3(1.58%) |
| Belgium | 2(1.05%) |
| Others | 6(3.16%) |
| North America | |
| the United States | 125(65.79%) |
| Canada | 1(0.53%) |
| South America | |
| Brazil | 4(2.11%) |
| Other Countries | |
| Not Specified | 42(22.11%) |
| Received year | |
| 2019 | 9(4.74%) |
| 2020 | 12(6.32%) |
| 2021 | 73(38.42%) |
| 2022 | 58(30.53%) |
| 2023 | 35(18.42%) |
| 2024 | 3(1.58%) |
Table 4A
| Clinical characteristics | Total [(N =167) %] |
|---|---|
| Gender | |
| Male | 2(1.20%) |
| Female | 161(96.41%) |
| Unknown | 4(2.40%) |
| Age, years | |
| ≥18Y & <50Y | 8(4.79%) |
| ≥50Y & <70Y | 33(19.76%) |
| ≥70Y | 24(14.37%) |
| Unknown | 102(61.08%) |
| Outcome | |
| Death | 3(1.80%) |
| Hospitalization | 23(13.77%) |
| Other Outcomes | 141(84.43%) |
| Area & Country | |
| Asia | |
| Israel | 2(1.20%) |
| Taiwan | 1(0.60%) |
| Others | 2(1.20%) |
| Europe | |
| Russia | 2(1.20%) |
| France | 2(1.20%) |
| Belgium | 2(1.20%) |
| Others | 5(2.99%) |
| North America | |
| the United States | 110(65.87%) |
| South America | |
| Brazil | 5(2.99%) |
| Other Countries | |
| Not Specified | 36(21.56%) |
| Received year | |
| 2019 | 8(4.79%) |
| 2020 | 21(12.57%) |
| 2021 | 62(37.13%) |
| 2022 | 42(25.15%) |
| 2023 | 32(19.16%) |
| 2024 | 24(14.37%) |
Table 4B
Table 4: Characteristics of reports with Alpelisib-related fatigue (A) and nausea (B) in patients with BC sourced from the FAERS database's (from the database's inception to December 31, 2024).
Correlation Analysis between Alpelisib and Fatigue/Nausea
The reporting odds ratios (RORs) for fatigue and nausea in patients with BC taking alpelisib compared to all other background drugs were 2.281 (95% CI: 1.953, 2.664) and 2.003 (95% CI:1.701, 2.360), respectively. The proportional reporting ratios (PRRs) for fatigue and nausea were 2.112 and 1.887, indicating a significant signal for AEs (Table 6). This suggests that the risk of fatigue and nausea in patients with BC treated with alpelisib is higher than in those treated with other drugs. The four-fold table for alpelisib versus the background drugs is presented in (Table 5 and Table 6).
| Alpelisib | All other drugs | Sums | |
|---|---|---|---|
| Fatigue | 190 | 5281 | 5471 |
| All other AEs | 1251 | 79308 | 80559 |
| Sums | 1441 | 84589 | 86030 |
Table 5A
| Alpelisib | All other drugs | Sums | |
|---|---|---|---|
| Nausea | 167 | 5195 | 5362 |
| All other AEs | 1274 | 79394 | 80668 |
| Sums | 1441 | 84589 | 86030 |
Table 5B
Table 5: Four-fold table of Alpelisib and background drugs.
| Report number | Adverse Event | PRR | ROR (95%CI) |
|---|---|---|---|
| 497 | hyperglycaemia | 110.482 | 157.202(132.378, 186.680) |
| 349 | diarrhoea | 2.951 | 3.453(3.030, 3.935) |
| 287 | rash | 7.585 | 8.987(7.790, 10.368) |
| 230 | fatigue | 2.112 | 2.281(1.953, 2.664) |
| 209 | blood glucose increased | 35.423 | 40.182(33.041, 48.865) |
| 202 | nausea | 1.887 | 2.003(1.701, 2.360) |
| 143 | decreased appetite | 3.751 | 3.994(3.288, 4.852) |
| 140 | weight decreased | 5.439 | 5.809(4.747, 7.109) |
| 125 | vomiting | 1.92 | 1.992(1.628, 2.437) |
| 122 | asthenia | 2.284 | 2.377(1.927, 2.932) |
Table 6: PRR and ROR of Alpelisib-associated the first 10 AEs in patient with BC in the FAERS database..
DISCUSSION
The safety and tolerability of PI3K inhibitors remain a persistent challenge. The first-generation agents, buparlisib and pictilisib, combined with fulvestrant, showed median PFS (mPFS) improvement, particularly in patients with PIK3CA mutations. However, the improvement was limited, and significant AEs occurred due to the broad target spectrum.
Buparlisib was prematurely discontinued in patients with poor tolerance. The most common AEs leading to discontinuation were elevated liver transaminase levels and depression due to the drug’s ability to cross the blood–brain barrier [8,20,22,23]. Additionally, pictilisib caused skin toxicity, hyperglycemia, and respiratory toxicity, which reduced patient tolerance and limited its therapeutic efficacy [9,21,25]. Given the toxicity of the extensive on- and off-target effects, the second-generation α-selective PI3K inhibitors have become the preferred choice for ongoing and future trials [26]. Taselisib combined with fulvestrant demonstrated a two-month increase in mPFS [10,25]. In the neoadjuvant setting, taselisib combined with letrozole significantly enhanced the Objective Response Rate (ORR) in patients with hormone receptor (HR) (+) /HER2(−) early BC [24,25]. Due to its long half-life and selective degradation of mutant p110α (not possessed by pictilisib and alpelisib), taselisib showed superior clinical activity in treating PIK3CA-mutaed BC with better tolerability than first-generation agents and manageable AEs, including gastrointestinal toxicity, fatigue, and hyperglycemia [10,24,27]. Furthermore, inavolisib combined with palbociclib and fulvestrant demonstrated a significant extension in PFS in a recent Phase III trial, accompanied by a lower proportion of patients discontinuing treatment due to AEs. Moreover, it exhibits the ability to selectively degrade mutant p110α, with higher subunit selectivity and overall kinase selectivity, potentially improving the therapeutic index of PIK3CA mutant tumors [27,28]. Toxic effects (grade 3/4 hyperglycemia, stomatitis, diarrhea, and rash) can be managed through supportive care and dose adjustments [11]. In contrast, alpelisib combined with fulvestrant nearly doubled the mPFS in BC with PIK3CA mutations. This outcome led to the US Food and Drug Administration (FDA) approval as the first and only PI3K inhibitor until now for patients with PIK3CA mutations, HR (+), and HER2 (-) advanced BC during or after receiving endocrine therapy [3,29–33]. However, the proportion of patients discontinuing treatment due to AEs was relatively high, and the most common AEs included hyperglycemia, diarrhea, rash, nausea, and fatigue [3,30,34]. Therefore, this study aimed to investigate the occurrence of fatigue and nausea during treatment with PI3K inhibitors and explore their potential causes.
Most PI3K inhibitors are ATP-competitive. The ATP-binding site of PI3K is located between the two kinase domains separated by a hinge region that is critical for inhibitor selectivity. The valine hinge residue is highly conserved across all class I PI3K and forms hydrogen bonds with the purine ring of ATP [7,35]. By occupying the ATP-binding site, PI3K inhibitors prevent ATP activated class I PI3Ks from converting PIP2 into PIP3, thereby halting the activation of downstream signaling pathways and disrupting cellular energy metabolism.
Fatigue is one of the most common AEs in patients with BC treated with PI3K inhibitors. Researchers have proposed that cancer treatment-related fatigue might be associated with the following processes: (1) Potential damage to the peripheral nervous system, including reduced energy metabolism and muscle fatigue; (2) Potential damage to the Central Nervous System (CNS), including inflammation, immune responses, and dysregulation of the hypothalamic–pituitary–adrenal axis; (3) Disruption of circadian rhythms and sleep deprivation; (4) Psychological factors, such as anxiety and depression; (5) Cardiovascular side effects; (6) Malnutrition due to gastrointestinal toxicity [16]. Nausea is one of the major AEs. Studies in mouse models have elucidated potential neurobiological mechanisms by which chemotherapeutic drugs induce nausea in patients: The ingested chemotherapeutic drugs are recognized as toxins by the body, activating enterochromaffin cells in the intestinal epithelium of mice and leading to a substantial release of 5-hydroxytryptamine. The signal is transmitted via the vagus nerve surrounding the enterochromaffin cells to the solitary tract nucleus in the brainstem and is received by neurons expressing the tachykinin gene (Tac1+). On the one hand, this activates the parabrachial nucleus, a center for aversive emotions associated with nausea; on the other hand, it activates the ventral respiratory group in the medulla oblongata, which may induce the motor behavior of retching by regulating the neurons responsible for the simultaneous contraction of the diaphragm and abdominal muscles in the CNS [36].
This is the first meta-analysis to reveal a significantly increased risk of fatigue and nausea associated with PI3K inhibitors treatment in patients with BC. The events and proportions of fatigue are presented (Table 2) with an RR (Figure 2), which indicated a significant increase in the risk of fatigue associated with PI3K inhibitors. However, the subgroup analysis indicated that most drugs only increased the risks of all-grade fatigue; while buparlisib was associated with a risk of grade 3/4 fatigue. Given that buparlisib notably affects the CNS, vigilance is warranted regarding the potential for high-grade fatigue to progress to psychiatric disorders in treated patients. This finding requires verification with a larger sample size. The risk of all-grade fatigue with taselisib showed no significant difference compared to the control group, which requires further validation and should be closely monitored for immunotoxicity-related AEs in patients. Additionally, in the subgroup analysis of patients with HER2(+) BC and early-stage BC, there appeared to be an improvement in the risk of fatigue; however, only one study was included for each subgroup, and both trials reduced the dosage and duration of medication compared to trials using the same drug. Therefore, it is difficult to attribute the risk differences of fatigue to HER2 status or cancer stage. Similarly, a larger sample size is required to validate these results[37].
The events and proportions of nausea are presented (Table 3) with an RR (Figure 4), which indicated a significant increase in the risk of nausea associated with PI3K inhibitors. Although the risk of all-grade nausea was significant, the SOLAR-1 trial contributed to a risk of grade 3/4 nausea. However, this trial constituted a small proportion of grade 3/4 nausea risk assessment among all the included trials. Therefore, the risk of nausea in patients with BC treated with PI3K inhibitors was significant but not severe, potentially not requiring additional assistance (such as nasal feeding, total parenteral nutrition, or hospitalization) to address insufficient intake but sufficient to impact the QOL of patients. In the subgroup analysis of patients with HER2(+) BC, the outcomes appeared to improve in the risk of nausea but required validation with a larger sample size.
Our study has certain limitations. First, this was a trial-level meta-analysis and lacked individual patient data; therefore, preventing adjustment for individual confounders. However, it is important to point out that this is inherent to meta-analyses of literature-based studies, and even individual patient data can carry significant bias, as accessible data are often limited to specific research groups and study types with high public health priority, leaving few opportunities for a pooled analysis. Second, fatigue and nausea are highly subjective symptoms, and patient reported outcomes would be ideal for evaluation according to QOL assessments. We used the AE data reported according to the NCI CTCAE grading system, which incorporates investigator subjectivity when grading the event, although the randomization and blinding processes help mitigate this bias. Third, different concomitant treatments, dosages, and cancer types in the included trials may account for heterogeneity. Fourth, multitarget inhibitors were excluded; therefore, these findings cannot be extrapolated to them. Fifth, except for alpelisib, other PI3K inhibitors for BC have not yet been approved for the market. We observed that buparlisib significantly increased the risk of grade 3/4 fatigue, consistent with the results of the original trials, which may be one of the reasons why it was not approved. Consequently, increased attention should be given to the increased risk of grade 3/4 nausea associated with alpelisib. In addition, inavolisib demonstrates a low risk of fatigue and nausea, and the rest of the reported toxicities are manageable, which makes it a promising future therapy for BC after adequate sample validation.
CONCLUSION
This meta-analysis revealed a significant association between the administration of PI3K inhibitors and an increased risk of all-grade and grade 3/4 fatigue, as well as all-grade nausea. However, PI3K inhibitors have shown considerable superiority of specific populations and improvements in patient outcomes in numerous clinical trials, an expanded sample size could be employed to investigate whether the incidence of fatigue and nausea remains stable when applied to HER2(+) or early stage BC populations, and to investigate whether inavolisib is associated with a more favorable profile of fatigue, nausea, and other AEs compared to Alpelisib in certain contexts. As the clinical use of these agents broadens, healthcare professionals must remain vigilant about the potential risks. In cases where high-grade nausea and declines in QOL are observed in the alpelisib-treated patients, appropriate pharmacological or other therapeutic measures should be employed, and aim to optimize patient outcomes.
ACKNOWLEDGEMENTS
No funds, or other support was received. Special thanks are extended to Jiuda Zhao for his invaluable assistance in this study.
COMPETING INTERESTS DECLARATIONS
The authors have no competing interests to declare that are relevant to the content of this article.
HUMAN ETHICS AND CONSENT TO PARTICIPATE DECLARATIONS
Not applicable.
REFRENCES
- Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229-263.
[Crossref] [Google Scholar] [PubMed]
- Giaquinto AN, Sung H, Newman LA, Freedman RA, Smith RA, Star J, et al. Breast cancer statistics 2024. CA Cancer J Clin. 2024;74(6):477-495.
[Crossref] [Google Scholar] [PubMed]
- André F, Ciruelos EM, Juric D, Loibl S, Campone M, Mayer IA, et al. Alpelisib plus fulvestrant for PIK3CA-mutated, hormone receptor-positive, human epidermal growth factor receptor-2-negative advanced breast cancer: final overall survival results from SOLAR-1. Ann Oncol. 2021;32(2):208-217.
[Crossref] [Google Scholar] [PubMed]
- Rugo HS, Lerebours F, Ciruelos E, Drullinsky P, Ruiz-Borrego M, Neven P, et al. RETRACTED: Alpelisib plus fulvestrant in PIK3CA-mutated, hormone receptor-positive advanced breast cancer after a CDK4/6 inhibitor (BYLieve): one cohort of a phase 2, multicentre, open-label, non-comparative study. Lancet Oncol. 2021;22(4):489-498.
[Crossref] [Google Scholar] [PubMed]
- Fruman DA, Chiu H, Hopkins BD, Bagrodia S, Cantley LC, Abraham RT. The PI3K pathway in human disease. Cell. 2017;170(4):605-635.
[Crossref] [Google Scholar] [PubMed]
- Hoxhaj G, Manning BD. The PI3K-AKT network at the interface of oncogenic signalling and cancer metabolism. Nat Rev Cancer. 2020;20(2):74-88.
[Crossref] [Google Scholar] [PubMed]
- Vanhaesebroeck B, Perry MW, Brown JR, André F, Okkenhaug K. PI3K inhibitors are finally coming of age. Nat Rev Drug Discov. 2021;20(10):741-769.
[Crossref] [Google Scholar] [PubMed]
- Campone M, Im SA, Iwata H, Clemons M, Ito Y, Awada A, et al. Buparlisib plus fulvestrant versus placebo plus fulvestrant for postmenopausal, hormone receptor-positive, human epidermal growth factor receptor 2-negative, advanced breast cancer: Overall survival results from BELLE-2. Eur J Cancer. 2018; 103:147-154.
[Crossref] [Google Scholar] [PubMed]
- Vuylsteke P, Huizing M, Petrakova K, Roylance R, Laing R, Chan S, et al. Pictilisib PI3Kinase inhibitor (a phosphatidylinositol 3-kinase [PI3K] inhibitor) plus paclitaxel for the treatment of hormone receptor-positive, HER2-negative, locally recurrent, or metastatic breast cancer: interim analysis of the multicentre, placebo-controlled, phase II randomised PEGGY study. Ann Oncol. 2016;27(11):2059-2066.
[Crossref] [Google Scholar] [PubMed]
- Dent S, Cortés J, Im YH, Diéras V, Harbeck N, Krop IE, et al. Phase III randomized study of taselisib or placebo with fulvestrant in estrogen receptor-positive, PIK3CA-mutant, HER2-negative, advanced breast cancer: The SANDPIPER trial. Ann Oncol. 2021;32(2):197-207.
[Crossref] [Google Scholar] [PubMed]
- Turner NC, Im SA, Saura C, Juric D, Loibl S, Kalinsky K, et al. Inavolisib-based therapy in PIK3CA-mutated advanced breast cancer. N Engl J Med. 2024;391(17):1584-1596.
[Crossref] [Google Scholar] [PubMed]
- Nunnery SE, Mayer I. Management of toxicity to isoform α-specific PI3K inhibitors. Ann Oncol. 2019;30:x21-x26.
[Crossref] [Google Scholar] [PubMed]
- Bower JE. Cancer-related fatigue—mechanisms, risk factors, and treatments. Nat Rev Clin Oncol. 2014;11(10):597-609.
[Crossref] [Google Scholar] [PubMed]
- Goedendorp MM, Andrykowski MA, Donovan KA, Jim HS, Phillips KM, Small BJ, et al. Prolonged impact of chemotherapy on fatigue in breast cancer survivors: A longitudinal comparison with radiotherapy‐treated breast cancer survivors and noncancer controls. Cancer. 2012;118(15):3833-3841.
[Crossref] [Google Scholar] [PubMed]
- Saligan LN, Olson K, Filler K, Larkin D, Cramp F, Sriram Y, et al. The biology of cancer-related fatigue: A review of the literature. Support Care Cancer. 2015;23(8):2461-2478.
[Crossref] [Google Scholar] [PubMed]
- Thong MS, Van Noorden CJ, Steindorf K, Arndt V. Cancer-related fatigue: Causes and current treatment options. Curr Treat Options Oncol. 2020;21(2):17.
[Crossref] [Google Scholar] [PubMed]
- Navari RM, Aapro M. Antiemetic prophylaxis for chemotherapy-induced nausea and vomiting. N Engl J Med. 2016;374(14):1356-1367.
[Google Scholar] [PubMed]
- Farrell C, Brearley SG, Pilling M, Molassiotis A. The impact of chemotherapy-related nausea on patients' nutritional status, psychological distress and quality of life. Support Care Cancer. 2013;21(1):59-66.
[Crossref] [Google Scholar] [PubMed]
- Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376.
[Crossref] [Google Scholar] [PubMed]
- Di Leo A, Johnston S, Lee KS, Ciruelos E, Lønning PE, Janni W, et al. Buparlisib plus fulvestrant in postmenopausal women with hormone-receptor-positive, HER2-negative, advanced breast cancer progressing on or after mTOR inhibition (BELLE-3): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2018;19(1):87-100.
[Crossref] [Google Scholar] [PubMed]
- Krop IE, Mayer IA, Ganju V, Dickler M, Johnston S, Morales S, et al. Pictilisib for oestrogen receptor-positive, aromatase inhibitor-resistant, advanced or metastatic breast cancer (FERGI): A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol. 2016;17(6):811-821.
[Crossref] [Google Scholar] [PubMed]
- Loibl S, de la Pena L, Nekljudova V, Zardavas D, Michiels S, Denkert C, et al. Neoadjuvant buparlisib plus trastuzumab and paclitaxel for women with HER2+ primary breast cancer: A randomised, double-blind, placebo-controlled phase II trial (NeoPHOEBE). Eur J Cancer. 2017; 85:133-145.
[Crossref] [Google Scholar] [PubMed]
- Martín M, Chan A, Dirix L, O’Shaughnessy J, Hegg R, Manikhas A, et al. A randomized adaptive phase II/III study of buparlisib, a pan-class I PI3K inhibitor, combined with paclitaxel for the treatment of HER2-advanced breast cancer (BELLE-4). Ann Oncol. 2017;28(2):313-320.
[Crossref] [Google Scholar] [PubMed]
- Saura C, Hlauschek D, Oliveira M, Zardavas D, Jallitsch-Halper A, de la Peña L, et al. Neoadjuvant letrozole plus taselisib versus letrozole plus placebo in postmenopausal women with oestrogen receptor-positive, HER2-negative, early-stage breast cancer (LORELEI): A multicentre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol. 2019;20(9):1226-1238.
[Crossref] [Google Scholar] [PubMed]
- Ellis H, Ma CX. PI3K inhibitors in breast cancer therapy. Curr Oncol Rep. 2019;21(12):110.
[Crossref] [Google Scholar] [PubMed]
- Patsouris A, Augereau P, Frenel JS, Robert M, Gourmelon C, Bourbouloux E, et al. Benefits versus risk profile of buparlisib for the treatment of breast cancer. Expert Opin Drug Saf. 2019;18(7):553-562.
[Crossref] [Google Scholar] [PubMed]
- Hanan EJ, Braun MG, Heald RA, MacLeod C, Chan C, Clausen S, et al. Discovery of GDC-0077 (inavolisib), a highly selective inhibitor and degrader of mutant PI3Kα. J Med Chem. 2022;65(24):16589-16621.
[Crossref] [Google Scholar] [PubMed]
- Song KW, Edgar KA, Hanan EJ, Hafner M, Oeh J, Merchant M, et al. RTK-dependent inducible degradation of mutant PI3Kα drives GDC-0077 (Inavolisib) efficacy. Cancer Discov. 2022;12(1):204-219.
[Crossref] [Google Scholar] [PubMed]
- André F, Ciruelos E, Rubovszky G, Campone M, Loibl S, Rugo HS, et al. Alpelisib for PIK3CA-mutated, hormone receptor-positive advanced breast cancer. N Engl J Med. 2019;380(20):1929-1940.
[Crossref] [Google Scholar] [PubMed]
- Gradishar WJ, Moran MS, Abraham J, Abramson V, Aft R, Agnese D, et al. Breast cancer, version 3.2024, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2024;22(5):331-357.
[Crossref] [Google Scholar] [PubMed]
- Loibl S, Poortmans P, Morrow M, Denkert C, Curigliano G. Breast Cancer. Lancet. 2021;397 (10286):1750-1769.
- Nunnery SE, Mayer IA. Targeting the PI3K/AKT/mTOR pathway in hormone-positive breast cancer. Drugs. 2020;80(16):1685-1697.
[Crossref] [Google Scholar] [PubMed]
- Society of Clinical Research of Oncology Medications of China Anticancer Association, Breast Cancer Expert Committee of National Cancer Quality Control Center, Boao Cancer Innovation Institute. Expert consensus on the clinical application of PI3K/AKT/mTOR inhibitors in the treatment of advanced breast cancer. Cancer Innov. 2022;1(1):25-54.
[Crossref] [Google Scholar] [PubMed]
- Mayer IA, Prat A, Egle D, Blau S, Fidalgo JA, Gnant M, et al. A phase II randomized study of neoadjuvant letrozole plus alpelisib for hormone receptor-positive, human epidermal growth factor receptor 2-negative breast cancer (NEO-ORB). Clin Cancer Res. 2019;25(10):2975-2987.
[Crossref] [Google Scholar] [PubMed]
- Zhang M, Jang H, Nussinov R. PI3K inhibitors: Review and new strategies. Chem Sci. 2020;11(23):5855-5865.
[Crossref] [Google Scholar] [PubMed]
- Xie Z, Zhang X, Zhao M, Huo L, Huang M, Li D, et al. The gut-to-brain axis for toxin-induced defensive responses. Cell. 2022;185(23):4298-4316.
[Crossref] [Google Scholar] [PubMed]
- Vanhaesebroeck B, Burke JE, Madsen RR. Precision targeting of mutant PI3Kα in cancer by selective degradation. Cancer Discov. 2022;12(1):20-22.
[Crossref] [Google Scholar] [PubMed]
Author(s) Info
1 Department of Oncological Surgery, School of Clinical Medicine, Graduate School of Qinghai University, Xining, China2 Department of Breast Disease Diagnosis and Treatment, Affiliated Hospital of Qinghai University, Xining, China
3 Department of Oncology, School of Clinical Medicine, Graduate School of Qinghai University, Xining, China
Received date: 08-Oct-2025 Editor Assigned: 13-Oct-2025 Reviewed: 20-Oct-2025 Revised: 03-Nov-2025 Published date: 10-Nov-2025
Citation: Sun J, Qiu T, Cui J, Shen G (2025) Risk of Fatigue and Nausea in Patients with Breast Cancer Treated with Phosphatidylinositol 3-Kinase Inhibitors: A Meta-Analysis Based on Randomized Controlled Trials. Med Chem Drug Discov.1:1.
Copyright: © 2025 Shen G, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
